Will Trump's wall between the U.S. and Mexico ever be built? Who knows? What are the political and economic ramifications of the wall? I haven't the wildest. Not my job. But, this is: the plague of opioid overdose deaths that we are now seeing, and our hopelessly misguided policy for dealing with it. (If you think "plague" is too strong a word, see my interview with DEA Special Agent Erin Mulvey, below.)
If a wall were in place, would it help fight the plague? Not alone. It might slow down, but not stop the waves of deadly non-prescription narcotics, which are constantly pouring in from Mexico. To put a dent in narcotic drug trafficking, the U.S. would need to focus on interdiction by air, land, and sea, and even this would not keep out all the narcotics that are killing Americans.
Yet, a wall alone, even if ill-conceived and largely ineffective, would still be a better plan to address the narcotic overdose epidemic that our current focus—counting the number of Vicodin pills prescribed by your dentist or doctor. While people are dying by the thousands from illegal opioids, the CDC is more concerned with restricting access to legal ones.
It would be hard to find a better example of 'unintended consequences' than what is now taking shape in the US. Instead of helping, our recent policy of severely limiting patient access to opioid pain medications can only make things worse for almost everyone. Addicts will be much more likely to die, because the alternatives to pills are far more dangerous than the pills, or even heroin, which many turned to when pills became unavailable.
And, life will be worse for ordinary people, all of whom will certainly experience severe pain during their lives. No matter how responsibly they use the drug, or how bad their pain is, patients with legitimate need for strong pain medications are increasingly being treated like addicts, simply for having the unmitigated gall to want a drug that is strong enough to give them relief. Worse still, doctors are becoming increasingly fearful of writing opioid prescriptions, even for long-time patients. They are afraid of losing their licenses.
This fiasco is brought to us courtesy of the CDC (mostly), as well as the DEA, and some medical associations, and arises from a distorted overreaction which made an already-bad problem worse. Lax opioid drug prescribing practices over the past two decades supposedly (1) caused many patients to became addicted, and died from overdoses of the pills, or from the heroin that replaced them. So the way to "correct" this was to push the pendulum so hard in the other direction that the chain snapped.
How well has this worked so far? Let's go with "terribly." First, the assumption that addiction arises primarily as a result of the legitimate use of legally prescribed opioids has been challenged. Second, since pills have been restricted, addicts are now using far more dangerous substitutes, such as fentanyl. If this trend continues, exactly two things will happen:
- There will be more deaths, not fewer.
- Patients who legitimately need the drugs will suffer.
The graphs below, one from Florida, and the other from Massachusetts, illustrate what is really killing opioid addicts.
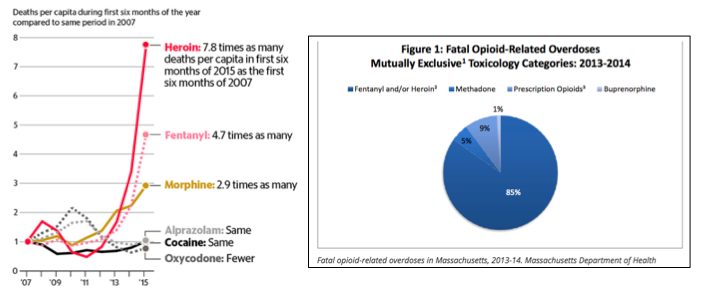
Sources: Left, Source: Florida Department of Law Enforcement. Right, Massachusetts Department of Health
On the left, the causes of opioid overdose deaths in Florida between 2007-2015 are given. Deaths per capita from oxycodone were about the same during the first six months of 2007 and 2015. But deaths from injectable opioids are 15-times higher (2) during the same time periods. Between 2013-2014 in Massachusetts, only 9 percent of opioid overdose deaths were due to pills, while 85% were due to heroin/fentanyl. Are pill overdoses killing addicts now? No. They are being killed by whatever they switched to after pills.
Any lingering doubts the origin of these drugs can be quickly tossed out the window, thanks to Special Agent Erin Mulvey of the New York City division of the DEA. Agent Mulvey kindly provided some eye-opening information:
JB: News stories have indicated that fentanyl is being made in China and then transported into the US through Mexico. Is this consistent with the DEA is observing?
EM: Yes. The news stories about fentanyl pouring in from Mexico are consistent with what the DEA is seeing. This is being driven by the Mexican drug cartels. They receive their fentanyl from China, but also make their own in labs located in Mexico. It is difficult to put a number on the amount of fentanyl coming across the border but considering the significant increase in seizures and overdoses, we can determine it has increased.
JB: What percent of the fentanyl that enters the US comes from Mexico?
EM: In NYC, kilos of fentanyl and fentanyl-heroin mixtures are being seized. The number of seizures of both (meaning both fentanyl alone plus mixtures of the two) in NYC has gone up by 2,000 percent compared to 4 years ago, with 95 percent of it coming through Mexico.
JB: What information do you have about fatal overdoses? What is responsible for the deaths?
EM: First, we know that about 80 percent of the people who recently started to use heroin had previously used prescription pain pills. According to the NYC Department of Health and Mental Hygiene, the number of overdose deaths in New York City went up 66 percent between 2010 and 2015. Of that number, 59 percent of the fatal overdoses involved heroin and 16 percent involved fentanyl.
JB: How do these data differ from what has been seen in the past in New York?
EM: Over the period 2005-2015, only 3 percent of all injectable overdose deaths involved fentanyl. Now it is 16 percent.
Since it could not be more than obvious what is really killing America' addicts, it is reasonable to ask why we are on a path that will do little good (and substantial harm), rather than focusing the real causes of overdose deaths.
In a sense, a wall is already in use, but it is a the wrong wall—one placed between patients and their doctors, thanks to misguided bureaucrats. And the 800-pound opioid molecule in the room keeps on killing.
What a mess.
Notes:
(1) Supposedly is correct. See: Scholten and Henningfield- "Negative outcomes of unbalanced opioid policy supported by clinicians, politicians, and the media." Journal of Pain & Palliative Care Pharmacotherapy. 2016
(2) I have combined all injectable narcotics to get this number. What the exact contribution of each drug is to the overdose statistics is often difficult to determine, and often irrelevant.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


