

This graph is a lie. But it's a lie of omission and it's misleading, because anyone examining this graph would conclude that people all of sudden started dropping dead from Valium (and other benzodiazepines) (1). Except they haven't.
The current masochistic war on drugs, uh, make that Americans, doesn't just pertain to Vicodin or Percocet. Getting a scheduled drug (like a sedative) is enough to make you need a sedative. In New York, you can't get a prescription for a restricted drug even one day early (2). If you're going to run out of Ambien (3) in the middle of your planned vacation, you may be S.O.L. (4). But enough about this.
The graph is not there simply to debunk a myth (5), but rather as a teaching tool for one of the main tenets of pharmacology—drug-drug interactions (6). This explains why Valium is sometimes dangerous and sometimes not.
First, the word benzodiazepine is thrown around a lot. I would be remiss in my duty as a chemist (7) if I didn't try to make at least some sense out of it.

The chemical structure of Valium. The red circle contains a 7-membered ring having two nitrogen atoms (a diazapine). The green circle contains a benzene ring. When fused with another ring (sharing a bond between them) the term benzo is used. All benzodiazepines contain this fused two-ring structure, and differ only by the absence or presence other atoms (e.g., the chlorine).
The term "drug-drug interaction" itself is misleading, which is why most people think that if you take a bunch of different medicines they somehow find each other in your body and do icky things to you. Not true. What really happens is that one drug will do something to the body—usually to the liver—that alters the blood level of the second drug, making them either higher or lower. Although there is no easy way to predict this a priori , there are easy lab tests to let you know early if this is going to be a problem with the drug you are trying to discover. There are also a few generalities. Certain drugs, especially, anti-fungal medications are notorious for affecting the levels of other drugs you might be taking (8).
For example, the common antifungal drug Diflucan (fluconazole) (9) comes with a list of 651 (!!) other drugs that it interacts with, including asthma drugs, antidepressants, antihistamines, cholesterol medications, analgesics... many more. You can add 900 dietary supplements and herbal remedies to that list as well. Some of these interactions are very dangerous. People have died from taking fluconazole with certain HIV drugs, antibiotics, and ulcer drugs, among others.
The mechanism by which these effects take place is similar to the reason that Valium can either deadly or safe—inhibition or induction of a critical class of liver enzymes called cytochrome P450 (CYPs). CYPs are ubiquitous, and have been found in all living organisms. There are an enormous number of subtypes (called isotypes), and they exist for one primary reason—metabolism, especially redox reactions.
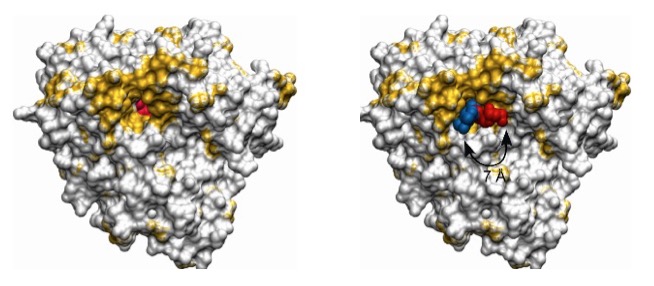
The x-ray crystallographic structures of a CYP protein (left) and the same protein bound to an antifungal drug (right). The drug is shown in blue and red. Note that the drug fits tightly into a cleft of the protein, turning it "off."
Source: PLOS
If one or more of the CYPs are inhibited by drugs, much higher, even lethal, levels of a normally safe drug can result. So can lower levels if the CYPs are activated, but this is less common. This is what really happens in a drug-drug interaction.
It is also one reason why Valium may or may not be deadly. In two case studies of suicide attempts using Valium, one person took 500 mg, and another took 2000 mg. Depending on the dosage, the number of pills consumed ranged from 50-400. (To put this in perspective, if you take that many aspirin, Advil, Tylenol, or NoDoz pills, you will end up being quite dead. Although both patients went into what was termed a "moderately deep coma," each of them woke up and were released from the hospital within two days. Clearly, Valium is a poor choice for suicide. It is too safe.
But not when you add alcohol. Unlike the anti-fungals alcohol does not strongly inhibit multiple CYPs; the effect is still there- just more subtle. One CYP isoform is called CYP2C19 and it plays a part in the metabolic fate of both alcohol and Valium, but in different ways. Alcohol is an inhibitor of CYP2C19 (Source: Adverse Drug Interactions: A Handbook for Prescribers), and Valium is a substrate of it (is metabolized by it). This means that the metabolism and thus, elimination of Valium will be slower in the presence of alcohol, and more will remain in the blood. The alcohol makes the Valium more dangerous.
There is an interesting a genetic analogy. Asians are more likely to have a genetic variant of CYP2C19, which makes it less efficient in the metabolism of a number of drugs, including Valium (10). So it is not surprising that there is a rule of thumb when prescribing benzodiazepines to Asian people: “Start low and go slow.”
The other reason that alcohol and Valium can be deadly is the same reason that opioids and Valium are. It is physiological, not pharmacological. All three drugs depress respiration, and the effects are additive. The more drugs, the more the effect. This is probably at least as important as the drug-drug interactions in this case.
So, the take home message here is that while Valium on its own is quite safe (11) do NOT combine it with other drugs. Then it becomes anything but.
So, if you don't get careless it is very unlikely that Valium will kill you. Don't know if I can say the same for this article.
Notes:
(1) There are about 15 benzodiazepines available in the US. The major differences between them are how quickly they work and how long they stay in the body.
(2) This is a mish mash function of laws, insurance company restrictions, and pharmacy policies. In New York, CVS won't let you order your Ambien online at one store and then switch the pickup to a more convenient store—something they routinely do for all prescriptions that are not scheduled. Or not. I was also told by them that it is left to the discretion of the individual pharmacist. Or maybe his dog. Yeah, go ahead and try to make sense out of this.
(3) The DEA keeps a 14-page list of scheduled drugs, should you have nothing better to do with your life.
(4) S.O.L. = Simply out of luck. Any of you who thought otherwise probably have dirty minds.
(5) What the graph doesn't say is that the vast majority of benzodiazepine deaths result from the combination of these with other drugs or alcohol. The combination is the killer. The upward trend in deaths from 2000-2013 is unquestionably a result of the concurrent rise in opioid use during the same time period.
(6) Drug-drug interactions are defined as "The combined effect of drugs taken concurrently. The result may be antagonism or synergism and may be lethal in some cases."
(7) Other chemist duties include: Dressing like you ran out of a burning hotel room (and thinking you look fine), pocket pen holders are no longer required, but recommended, and, unfortunately these days, looking for a job. Having things hanging out of your nose is optional. Chemists are not a glamorous bunch.
(8) The mechanism that causes these interactions is the same one makes grapefruit juice plus certain drugs a bad idea. The offending chemicals in grapefruit juice are called furanocoumarins. The are also CYP inhibitors.
(9) The suffix -azole is a dead giveaway. They are not only very likely to be anti-fungal drugs, but also belong to the subclass of antifungals that is the worst offender—the azoles.
(10) Some Asian people have a "double whammy," and it's all about genetics. A large percentage (about half, depending on geography) have low levels of the enzyme acetaldehyde dehydrogenase, which is responsible for the second of two steps in the metabolism of alcohol. When step #2 does not occur, acetaldehyde, which is quite toxic, accumulates, and this makes you quite ill. Some Asian people cannot drink any alcohol at all because of this.
(11) Safe as used in this article refers to acute dosages. Other factors such as dependency and addiction, and withdrawal are issue that are not relevant to this discussion.
