It's time for the Centers for Disease Control and Prevention to withdraw this page to correct its many errors and distortions. A principal author of the 2016 CDC Guidelines on the prescription of opioids to adults with chronic pain is responsible for many of these errors. Richard Lawhern (pictured) addressed these mistakes in this open letter.
As a volunteer patient advocate, I do my best to stay current on declarations of the US Centers for Disease Control and Prevention, concerning the treatment of acute and chronic pain. Thus I recently reviewed the CDC "Get Informed" page on prescription opioid basics [https://www.cdc.gov/rxawareness/information/index.html]. In my view, a better description of the page might be "get misinformed".
It is time for CDC to withdraw this page to correct its many errors and distortions. As a principal author of the 2016 CDC Guidelines on the prescription of opioids to adults with chronic pain, Dr. Debra Houry is responsible for many of these errors and is thus addressed in this open letter. In the order that these errors occur, I noted the following.
Errors in Science
While a few patients experience increased sensitivity to pain when managed for long periods on high doses of prescription opioids, this is a relatively rare phenomenon. [1] We have no medical science concerning any proposed mechanism by which such sensitivity occurs. There are no data other than highly dubious animal model studies to demonstrate that any such thing as "opioid-induced hyperalgesia" even exists. [2]
Interjection of Hype
The CDC writes:
"Overdose deaths involving prescription opioids were more than four times higher in 2018 than in 1999. In 2018, almost 32 percent of all U.S. opioid overdose deaths involved a prescription opioid. Even though the number of overdose deaths involving prescription opioids decreased in 2018, more than 232,000 people have died in the United States from overdoses involving prescription opioids since 19991. Overdose is not the only risk related to prescription opioids. Anyone who takes prescription opioids can become addicted to them."
My response to these assertions is as follows:
- The term "overdose deaths involving prescription opioids" seems to be a deliberate cherry-picking of evidence, to overstate the role of legitimately prescribed opioid pain relievers. Reality is far more ambiguous.
- There is evidence from multiple published studies that when prescription opioids are found in a postmortem blood tox screen, they are almost always accompanied by non-prescribed or illegal opioids and alcohol. [3, 4] Our so-called opioid crisis is largely one characterized by patients self-medicating by poly-pharmacy due to under-treatment of their pain, plus addicts who have never had a doctor's prescription.
- The idea that anyone who takes prescription opioids can become addicted to them is simply an outright damned lie! As we are informed by no less an authority than Dr. Nora Volkow and her co-author Dr. McMillan of the National Institute on Drug Abuse, “addiction is not a predictable outcome of prescribing,” and is in fact quite rare even among patients with identified risk factors that may increase vulnerability to substance abuse disorder. [5]
- The fraction of opioid-naive patients prescribed opioids after surgery who are later diagnosed with substance use disorder is on the order of 0.6%. Studies demonstrating this reality have assessed medical insurance records of over 1.5 million patients. [6] Such numbers almost certainly represent an upper limit, given that the diagnoses are most often made by general practitioners who have no training in the assessment of addiction, and who may render the diagnosis to justify discharging patients whom they regard as a risk to their license because of the hostile regulatory environment.
Misreading of Trials Outcomes
Many of the CDC’s listed alternatives to opioid analgesics fundamentally lack scientific support. The Agency for Healthcare Research and Quality released a systematic outcomes review in June 2018 for non-invasive and non-pharmacological treatments in chronic pain. [7] It addressed over 20 identified therapies in five common types of chronic pain.
Only about 220 from more than 5,000 published trials survived quality review. Medical evidence was evaluated as "weak" in over 100 of the surviving trials. The degree of improvement in pain or quality of life was marginal and temporary. NONE of these trials addressed alternatives as replacements for opioids. But the CDC web page proposes to use them in replacement roles. It may not be going too far to suggest that this proposal is medical malpractice of a high order and may become legally actionable by patients whom CDC has harmed.
The CDC also references its own CDC-Wonder database as a source for their analysis of overdose data. [8] However, the authors of this material fail to go beyond generalities that support their politically pre-determined anti-opioid agenda. In contrast to CDC’s unscientific misrepresentation of the data, independent investigators have much more deeply examined the relationship between opioid prescribing rates and opioid overdose-related mortality. [9, 10]
The following is a State by State plot of prescribing versus opioid overdose-related mortality data from the CDC-Wonder database.
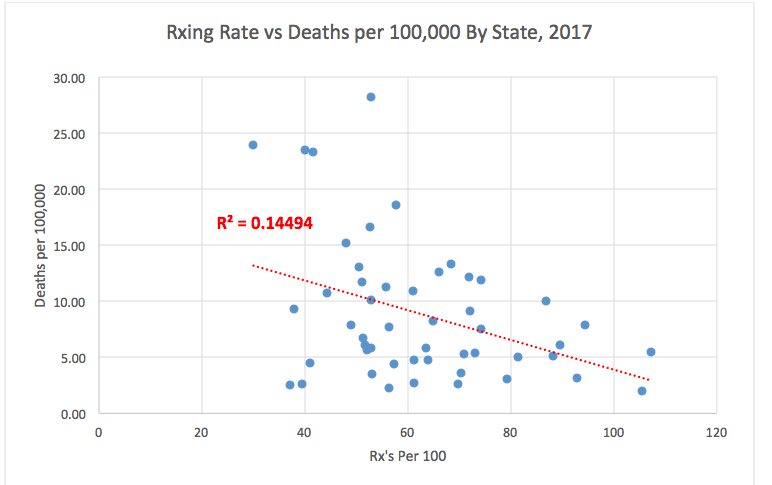
Opioid Overdose-Related Mortality versus Prescribing Rates (ICD Cause of Death Codes X42, X62, T40.0-T40.6)
This chart is typical of plots over the past 17 years. It demonstrates no correlation whatever between prescribing rates and overdose mortality. It also demonstrates a general trend toward lower opioid-related overdose mortality rates in States where prescribing rates are highest. The CDC has at least three times refused even to look at the data sets which generated this plot, in response to my previous inquiries. Readers of this article are welcome to a copy of the data, by request in comments.
It is time that CDC woke up and smelled the coffee. We have a genuine opioid "crisis" in the US in ever-rising opioid addiction and overdose rates. But the source of this crisis was not originally and is not now prescribing by medical providers to their patients. The supposed contribution of medical prescriptions gets lost in the noise of illegal street drugs.
The public positions CDC has assumed on this important issue are contradicted by their own data!
References
[1] Andrea Trescot, MD, in “Don’t Forget People Living in Pain: War on Opioids and Chronic Pain Patients during COVID-19” Cato Institute Panel Discussion, May 20, 2020 https://www.cato.org/events/dont-forget-people-living-pain-how-war-opioids-causing-chronic-pain-patients-unnecessary?fbclid=IwAR2FqU9SXqrfGzvEY2SVgbpYg_jYW-6KzZADYO2pG_o72C6UXvjwGZQ6dSM
[2] Donald C Harper, MD, “Misuse of ‘Hyperalgesia’ to Limit Care - Throwing the baby out with the bathwater” Practical Pain Management, V10, Issue 8, March 7, 2011
[3] Blake Dodge, “Only 1 Percent of People Become Chronic Opioid Users After Hospital Prescriptions for Injuries, Study Shows“ Newsweek Magazine, September 4, 2020. https://www.newsweek.com/only-1-percent-people-become-chronic-opioid-users-after-hospital-prescriptions-injuries-study-1471242
[4] Pat Anson, “Prescription Opioids Play Minor Role in Massachusetts Overdoses” Pain News Network, June 3, 2019
[5] Nora D Volkow, MD and Thomas A McLellan, Ph.D., “Opioid Abuse in Chronic Pain — Misconceptions and Mitigation Strategies” . NEMJ 2016; 374:1253-1263 March 31, 2016]. http://www.nejm.org/doi/full/10.1056/NEJMra1507771
[6] Gabriel A Brat, Denis Agniel, Andrew Beam, Brian Yorkgitis, Mark Bicket, Mark Homer, Kathe P Fox, Daniel B Knecht, Cheryl N McMahill-Walraven, Nathan Palmer, Isaac Kohane, “Postsurgical prescriptions for opioid naive patients and association with overdose and misuse: retrospective cohort study”, BMJ 2018;360:j5790
http://www.bmj.com/content/360/bmj.j5790.long
[7] Skelly AC, et al. “Noninvasive nonpharmacological treatment for chronic pain: a systematic review”. Prepared for AHRQ, HHS, Publication No.18-EHC013-EF, Rockville, MD, June 2018 [Updated June 2019]
[8] “Wide-ranging online data for epidemiologic research (WONDER). Atlanta, GA: CDC, National Center for Health Statistics; 2020. Available at http://wonder.cdc.gov.” [quoted from [https://www.cdc.gov/rxawareness/information/index.html].
[9] Jacob Sullum, “Opioid Death Rates Are Not Correlated With Prescription Rates Across States” Reason, 5.14.2018, https://reason.com/2018/05/14/opioid-death-rates-are-not-correlated-wi/
[10]. Richard A. Lawhern, Ph.D., “Stop Persecuting Doctors for Legitimately Prescribing Opioids for Chronic Pain”, STAT News, First Opinion, June 28, 2019, https://www.statnews.com/2019/06/28/stop-persecuting-doctors-legitimately-prescribing-opioids-chronic-pain/
