It is only logical that if someone makes the same mistake once or twice it might be wise to stop and think. But perhaps that is giving the CDC and FDA too much credit. The agencies seem to expect that if they continue to make the same mistake over and over perhaps they will finally get it right.
Not so, according to Frances Robles writing in today's New York Times. We continue to play "drug whack-a-mole" and are astonished when another mole keeps coming up in a different place. Basic concepts, such as human nature and unintended consequences seem to be lost upon our elected official and bureaucrats, so we are seeing a different flavor of the same problem popping up once again This time the flavor is a favorite from the past - methamphetamine. The drug is making a huge comeback, and no one should be the least bit surprised (Figure 1).
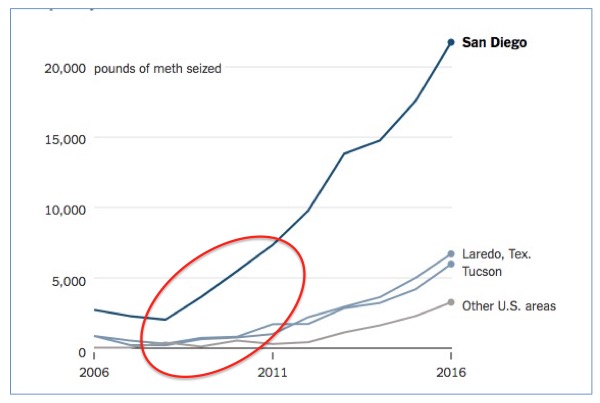
Figure 1. Methamphetamine seizures (pounds) in the US 2006-2016. Graph (modified): Sahil Chinoy. N.Y. Times Source: U.S. Customs and Border Protection
Hmm. A rapid increase in a drug use starting around 2010. Where might we have seen this before? Could it be here? Look at the red oval I added in Figure 2. Is history repeating itself?
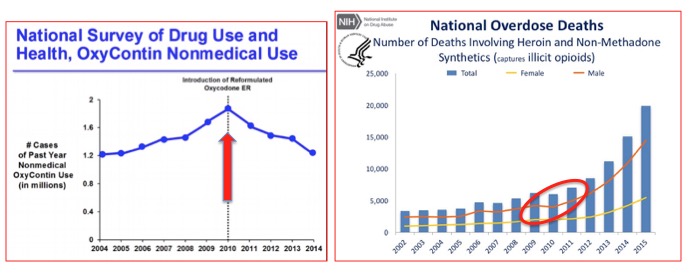
Figure 2. Overdose deaths from heroin soared in 2010, right after abuse-resistant OxyContin was approved. Coincidence? No.
It sure looks that way. An unintended consequence of the reformulation of OxyContin (1) in 2010 was an immediate surge in heroin deaths. Although no one can blame Purdue Pharma (2) for reformulating its product, there was a valuable lesson to be learned - if an abused drug becomes more difficult to obtain, users will switch to something else. And they sure did. It was this (presumably) well-intentioned move that ushered in today's so-called "opioid crisis." (3)
Then, to make matters worse, the CDC poured gasoline on the fire with more than a little help from their arsonist friends at the Physicians for Responsible Opioid Prescribing (PROP). Over the past few years, there has been a massive effort to cut opioid prescriptions to reduce overdose deaths. Did it work? The first part, yes. The second part, not so well. (Figure 3)
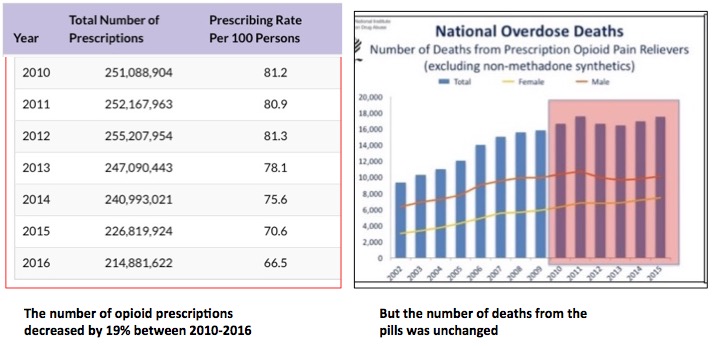
Figure 3. Although the number of opioid prescriptions decreased by 19% from 2010-2016 (source: CDC) deaths from pills remained unchanged (source: NIH), while at the same time deaths from heroin shot up (Figure 2).
So it's pretty safe to say that the harder it becomes to get opioid pills, either due to market forces, policy changes, or both, that the result has been even more deaths from heroin/fentanyl (Figure 2). Can you say "dismal failure?" (4)
Given human nature, as well as the nature of addiction, it should come as no surprise that as opioid drugs became scarce, another drug "stepped in" to fill the void. And it should be even less of a surprise (and more than a little ironic) that today's surge in meth is largely due to another stupid policy. In 2006, in a misguided effort to stop home "meth cooking," the FDA ordered Sudafed to be removed from pharmacy shelves (5). All this accomplished was to inconvenience allergy sufferers and (and predictably) prompt chemists to come up with a better method for making the drug. (See: Why Sudafed Is Behind The Counter: A Meth Chemistry Lesson.) The chemists succeeded admirably. Need proof? Here's plenty:
"I have been involved with meth for the last 25 years. A wholesale plummet of price per pound, combined with a huge increase of purity, tells me they have perfected the production or manufacturing of methamphetamine... They have figured out the chemical reactions to get the best bang for their bucks.”
Steven Bell, DEA spokesman
And now, about 6,000 people are dying from methamphetamine per year, not terribly different from the number who die from opioid pills (alone).
Let's sum up:
- The approval of abuse-resistant OxyContin opened the heroin/fentanyl spigot.
- The CDC-inspired crackdown on opioid pills opened it further; fewer pills were prescribed but this had no impact on deaths from the pills.
- Far more people are dying from overdoses now than in 2010.
- The scarcity of opioid pills also drove people to abuse methamphetamine.
- Methamphetamine is now easier to make and purer because the removal of Sudafed from pharmacy shelves in 2006 forced chemists to find a better way to make it. They did.
- More people are now dying from methamphetamine.
- Connect the dots.
Lessons un-learned:
- People are going to abuse drugs or alcohol. Period.
- There is very little that can be done about it.
- When drugs are restricted or prohibited, users will switch to something else.
- The "something else" will almost always be worse.
- Our drug policies are responsible for much of this mess.
Words fail me, so let's try music instead.
"When will we ever learn?"
Pete Seeger, "Where have all the flowers gone." 1955
Never, it would seem.
NOTES:
(1) Prior to 2010 OxyContin could be ground up to give a very high dose of oxycodone, which could be smoked or injected. The new formulation turned into a useless gum when users tried to grind it up. OxyContin use dropped rapidly once the new formulation was approved. Ironically, OxyContin was the primary driver of opioid addiction over the past two decades, and its reformulation was the primary driver of increased heroin usage.
(2) Although Purdue may not deserve blame for the unintended consequences of its formulation research, they have taken $650 million worth of blame (fine) and this isn't over.
(3) No - it's not a crisis at all. It is a manufactured crisis. Opioid pills (alone) kill about 5,000-10,000 people per year, roughly the same number as die in bicycle-related accidents. About 100-times more people are killed per year from smoking.
(4) When you add in the suffering of pain patients who are having their meds reduced or taken away, the failure becomes far worse.
(5) To buy Sudafed you must present a photo ID to the pharmacist. There is also a monthly limit on the quantity you can get.
