
Evidence-based medicine, it seems commonsensical; who could argue about using the best evidence available to make treatment decisions? The difficulty, of course, is that the evidence comes from studies of large populations, often expressed in terms of average responses; and as a clinician, you want to tailor the care to the one member of the population in front of you, your patient. How do you reconcile population-based evidence with the desire for personalized care?
“The premise of traditional research is to put a treatment at the center of consideration and decide, Is this treatment helpful for an average patient? Trouble is, there aren’t very many average patients out there, and I, like most people, am not an average patient.”
—Seth Morgan, neurologist, multiple sclerosis patient, and patient advocate
The gold-standard of therapeutic evaluation remains the randomized controlled trial, whose primary goal is to identify causation, using this drug or that procedure resulted in this outcome. The control group is meant to capture all the variables, but they rarely do, after all, in the complex biologic systems that we are, there are unknown unknowns. The problem is further compounded by the fact that the treatment results are rarely binary yes or no, they form a continuum of responses and for each place on the continuum different patient variable are identified. When you look at the population's "average response," it is accompanied by confidence intervals, a way of describing the variety of responses and patients, it represents the heterogenicity of the therapeutic effect.
The heterogenicity of outcomes can be altered by at least four factors, the baseline risk, the individual response to treatment, their “vulnerability” to adverse effects, and patient and societal preferences. Just a moment’s reflection will show that heterogenicity of outcomes is the rule, not the exception. For clinicians, the problem is, how similar is the patient in front of me to the population studied? That simple sentence belies a more profound concern as to what constitutes similarity.
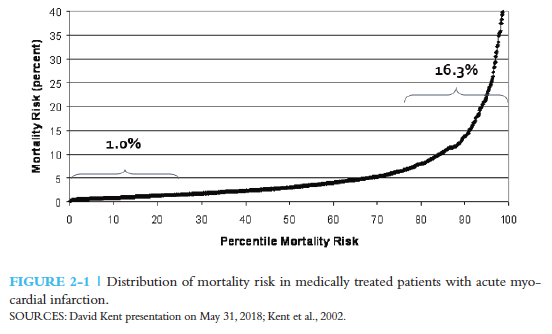 A discussion at the National Academy of Medicine doesn’t answer the question but provides a bit of guidance. It is reasonable to argue that when the outcome varies across sub-groups, the tradeoff between benefits and harm varies. In this graph showing the risk of death after myocardial infarction, only 20% of patients had risk higher than the population average of 6%; and even within their ranks, there was considerable variation. The majority of patients had a risk below average. The trick is to be able to identify the top tier from the majority. A similar diversity of outcomes can be found when looking at harms or complications of the proposed treatment. Population averages “often over-estimate the benefit in most patients and may obscure the harm in many others.” So the first solution in guiding the care of the individual is to regroup the data based on a patient’s risk and apply the same risk stratification to your patient.
A discussion at the National Academy of Medicine doesn’t answer the question but provides a bit of guidance. It is reasonable to argue that when the outcome varies across sub-groups, the tradeoff between benefits and harm varies. In this graph showing the risk of death after myocardial infarction, only 20% of patients had risk higher than the population average of 6%; and even within their ranks, there was considerable variation. The majority of patients had a risk below average. The trick is to be able to identify the top tier from the majority. A similar diversity of outcomes can be found when looking at harms or complications of the proposed treatment. Population averages “often over-estimate the benefit in most patients and may obscure the harm in many others.” So the first solution in guiding the care of the individual is to regroup the data based on a patient’s risk and apply the same risk stratification to your patient.
Another approach begins with the assumption that similar patients have similar benefits or harms. Heterogenicity certainly can create different subgroups in the category of harm as easily as it does benefit. Analyzing a clinical trial can provide you with two measures, one describing who may benefit, the other, who may be harmed. With this information in hand, a formula describing net benefit can be calculated from the patient’s particular variables. No such tools are currently available.
What Is A Doc Supposed To Do?
The bottom line is despite our best efforts, data-driven evidence-based medicine is difficult to apply. The heterogenicity of effect is responsible for many of the contradictory conclusions we have from studies, especially nutritional studies. While there are promising statistical manipulations on the horizon, our best algorithms are to be found in the physicians caring for us. A great deal of the buzz around AI is about its diagnostic acumen where it is just as good or slightly better than us; what is needed is help in identifying the best treatment for the patient across the desk, and in that area, AI has not been as successful.
Source: Caring for the Individual Patient: Understanding Heterogenous Treatment Effects National Academy of Medicine
