A recent analysis of COVID-19 and the 2020 wildfires in California, Oregon, and Washington estimated increases in COVID cases and mortality of about 20% associated with increased levels of fine particulate matter (PM2.5) based on satellite smoke observations. The study caught my eye for several reasons: PM2.5 is not “smoke,” the COVID-19 increases were not statistically significant, and a much simpler and transparent analysis of their data yielded different results. Here’s what I found.

The Agent. The assumption behind this paper is the equivalence of wildfire “smoke” and PM2.5, as monitored and regulated by the EPA. Smoke is a panoply of products of incomplete combustion, including oxides of nitrogen and various hydrocarbons, many of which have been found to exert adverse health effects. Wood smoke is laden with carbon compounds but contains essentially no sulfur. PM2.5 is a mixture of many types and size ranges of airborne particles of varying toxicity whose sole commonality is collection by a sampling filter. Sulfur compounds comprise a major portion of PM2.5 mass; the carbon compounds typically found in smoke contribute much less.
The patterns of wildfire smoke were obtained optically from satellite images, while human health effects have been attributed to ground-based particulate mass. The lack of data on ground-based concentrations of toxic combustion compounds emitted in the wildfire areas necessitates their assumption that wildfire “smoke” and PM2.5 are the same – they are not, and this is a fatal flaw in the analysis.
The Analysis. Their analysis compared the percentage changes in COVID cases and deaths on wildfire days with non-wildfire days in relation to changes in PM2.5 on those days. The study pooled 61 wildfire days (based on smoke observations) for 92 counties with the required data. They reported
- Eighty cases per million population on wildfire days and 69 on non-wildfire days, an excess of 16%.
- 1.23 deaths per million population on wildfire days and 1.0 on non-wildfire days, an excess of 23%.
Given the substantial variations in the mean values, these small differences are far from statistical significance. [1] Since the national peak daily infection rate is about 750 cases per million population, their use of the phrase “substantial exacerbations” seems unwarranted.
A Simpler Analysis
Harvard, the source of the study, has posted a dashboard presenting PM2.5 levels with and without wildfires, numbers of wildfire days, and mean incremental changes in COVID-19 case and death counts for each county. Using their data, I derived average daily case rates comparable to other public health statistics. The mean daily excess COVID-19 case rate for wildfire days was 41 per million + 8.6.
There are very substantial variations among these 92 counties. With a population of 10 million, about 20% of the total affected study population, Los Angeles showed a decrease of 10,737 cases over the 61 wildfire days, a daily rate of -25.9 per million population. By contrast, the daily case rate in Jefferson County, Oregon, with 20,000, increased by about 60 per million people. For comparison with the wildfire levels, the regional average case rates were about 100 per million.
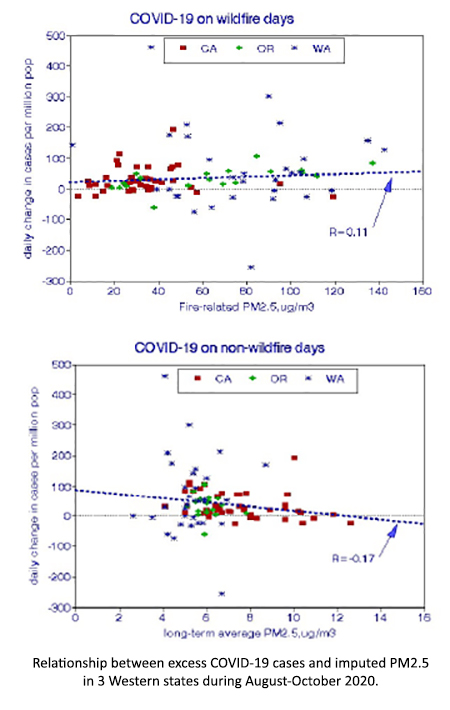
The relationship of wildfires with cases based on linear regression shows large positive and negative outliers. At the EPA ambient PM2.5 standard of 12 μg/m3, the risk would be 12% but not statistically significant. The corresponding relationship with COVID-19 deaths (not shown) was negative and insignificant. The data from Washington State are slightly higher than the others. Deleting the two outlying counties yielded a statistically significant relationship, but 95% of the variance in increased COVID cases remained unexplained.
As a counterfactual example, I regressed the excess COVID-19 cases against PM2.5 on non-wildfire days, intended to estimate previous long-term exposures that might have been associated with previous co-morbidity. That relationship was negative.
Discussion The underlying premise is that exposure to greater PM2.5 levels during wildfire episodes increased rates of COVID-19 infection. Air pollution impacts health in two ways.
- Acute effects (over several days) are limited to previously impaired elderly individuals with exposure to any of several pollutants as well as heat stress [2], but COVID-19 cases have been widely distributed across a wide range of age groups.
- Chronic responses require long-term accumulated reactions in the lung that are typically carbonaceous. There is little physiological support in the literature for equating the increased carbon exposure of smoke with COVID-19 infections. The available data indicate that smokers are less likely to develop severe COVID-19 disease requiring hospitalization.
I conclude that COVID-19 cases and deaths were significantly elevated on wildfire days in California, Oregon, and Washington in 2020, but the corresponding increased ambient PM2.5 levels were not the cause.
[1] I evaluated statistical significance as follows. The paper reported mean, maximum, and minimum values of cases and deaths on wildfire and non-wildfire days, but not standard deviations. I took the difference between maximum and minimum as equal to 6 standard deviations (99% level) and computed standard errors of means based on the numbers of days involved. Those values were 20 cases and 0.59 deaths per million. The corresponding t values were thus 11/20 and 0.23/0.59, a significance level of about 60%.
[2] Inferring frail life expectancies in Chicago from daily fluctuations in elderly mortality. Inhalation Toxicology DOI: 10.3109/08958378.2013.804610.
Source: Excess of COVID-19 cases and deaths due to fine particulate matter exposure during the 2020 wildfires in the United States. Sci Advances DOI: 10.1126/sciadv.abi8789.
