
Is it possible to get through even one day without reading something about opioids in the headlines? Pretty much, no. So, I would have ignored this one except for two reasons. First, there is something very un-cool about giving painkilling drugs to help sled dogs win a race, but this is just what happened in the 2017 Iditarod Trail Sled Dog Race (1). Dallas Seavey, a four-time winner of the race, has been accused of giving some of his dogs a painkilling drug called tramadol, a charge Seavey denies.
Second, tramadol is an interesting drug. It's not a typical opioid and it may be the least bad alternative for people who have pain and need medication. Tramadol (brand name Ultram) also provides an extraordinary example of one of the key principals of pharmacology, the pharmacophore—the portion(s) of a drug molecule that, when taken together, are responsible for the action of the drug.
Tramadol is classified as an atypical opioid; it has some properties of morphine, but also lacks others. It's also a rather good (but imperfect) pain medication and is on the DEA list of controlled substances. But it is not scheduled (restricted) the same way that Percocet is. The agency categorizes it as a Schedule IV narcotic, which places in a far less restrictive category. According to the DEA, "Substances in this schedule have a low potential for abuse relative to substances in Schedule III." Other common drugs that are Schedule IV are sleeping pills and/or sedatives, such as Valium, Xanax, and Ambien.
American Council friend, Dr. Aric Hausknecht, a pain management specialist and neurologist, who has contributed to our knowledge and writings on pain and pain drugs says,
"Tramadol is a great medication. It is very effective, has few side effects, and is well tolerated but I rarely prescribe it because there are so many potential interactions with other meds such as antidepressants and most of my chronic pain patients are taking these types of medications (in addition to opioids)."
Aric Hausknecht. M.D.
In today's climate, where getting pain medications can be very difficult, it is surprising that the drug isn't even more restricted. But does it belong in a restricted class at all? And, if so, why Schedule IV? In contrast to all the nonsensical laws, regulations, and lies that surround Vicodin, etc, there is actually some sound science here. More on that later. First, a tramadol lesson. It is actually more interesting than you'd think.
Upon first glance, tramadol appears to have little in common with another opioid, morphine, at least based on the chemical structure of each drug. They look rather different (Figure 1).
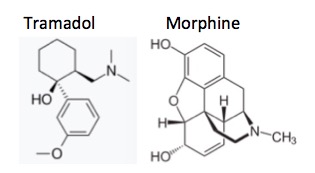
Figure 1. The chemical structures of tramadol (R) and morphine (L). Night and day?
But if you "map out" and compare the pharmacophores of the two, things start to look a bit different (Figure 2). The pharmacophores of the two molecules do bear some similarity to each other.
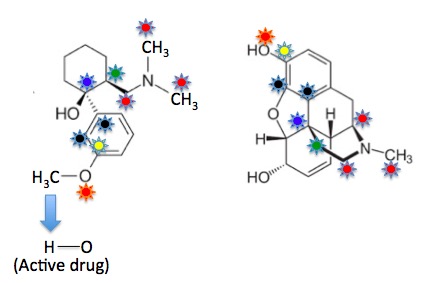
Figure 2. The chemical structures of tramadol (R) and morphine (L) with mapping of the pharmacophore. Now similarities begin to appear. The colored stars represent structural units that are common to both molecules.
Here is a description of the shared pharmacophore of both drugs:
- There are three carbon atoms (red stars) attached to the nitrogen atom of each molecule.
- These atoms are connected by a single atom (green star) to a tertiary carbon atom (a carbon atom which has four non-hydrogen atoms bound to it, blue stars).
- The carbon atom with the blue star is attached to a benzene ring.
- There is a hydroxyl group (OH, orange stars) at a position on the benzene ring two atoms from the blue star (also called meta, black stars). The hydroxyl group is essential.
Now, the similarity of the two pharmacophores of the two molecules becomes intriguing.
Those of you who have gotten this far and have managed to avoid some sort of life-support system may notice that something doesn't quite add up. In tramadol (Figure 2, left) the carbon bearing the yellow star is not connected to a hydroxyl (OH) group; but rather to an oxygen atom bound to a methyl group (OCH3 is called methoxy). These two groups are very different physically and pharmacologically. But I just said that the hydroxyl group on the yellow-starred carbon is essential for opioid activity, yet tramadol is still a pain drug. What's going on?
The answer is your liver. Methoxy groups that are attached to benzene rings are very yummy to your liver enzymes. The methyl group is rapidly "chewed off," forming the hydroxy group. This means that tramadol is not a drug at all, but rather a pro-drug—a compound that is pharmacologically inactive until processed by the body, which then converts it into the active drug (2).
And, since I have no life, I then deleted all of the "irrelevant" (3) atoms in each molecule, leaving only the pharmacophores of each, and then lined them up in the same direction. Now the similarity becomes striking. This is as good a demonstration as you'll see how seemingly dissimilar drugs can actually be very similar, both structurally and biologically, when you look at them in a different way (Figure 3).

Figure 3. The pharmacophores of tramadol (L) and morphine (R) with the rest of the atoms stripped away. They are essentially identical. It is no wonder that tramadol is considered to be an opioid.
So, at least theoretically, it makes some "sense" to give tramadol to dogs that pull sleds. Opioids are analgesics—drugs the relieve pain. Pain is a natural response to injury - the body's way of telling us to take it easy. If a drug blunts the pain response then a dog that might normally "take it easy" could be more likely to keep going, risking further injury. You don't have to be a PETA maniac to have problems with this.
Finally, the reasoning behind tramadol's Schedule IV status actually makes some sense scientifically. When tramadol was approved in 1994 it was not scheduled at all because of its low abuse potential relative to oxycodone, hydrocodone etc. But in 2013 the drug found its way onto the DEA Schedule IV list for three primary reasons.
- Needless to say, there are reports of tramadol being abused, even though its abuse potential is estimated to be only 10% that of morphine. Other recent studies have shown that at very high doses it can produce an "opioid high." (4)
- As Dr. Hausknecht mentioned above, tramadol has a number of drug-drug interactions, some of which can be very serious, even fatal. One is called Serotonin Syndrome, where abnormally high levels of serotonin are found in the blood. It is usually caused by a drug (such as tramadol) potentiating the action of a serotonin drug like an antidepressant.
- Patients have reported some pretty bad withdrawal symptoms after they've been on the drug for a while. This does not mean that they had become addicted.
Once again we have an example of the difficulty of the pharmacological treatment of pain. Tramadol is a pretty good drug but is still flawed. Everything else is just worse.
NOTES:
(1) The Iditarod is a 1-2 week dog sled race which runs from Settler's Bay to Nome, a distance of about 1,000 miles. You have to be out of your mind to do this. Wind chills of -100º F have been recorded.
(2) This process is called oxidative dealkylation. It involves the removal of one of the three hydrogen atoms of the methyl group, which is performed by a set of liver enzymes called cytochrome P450 oxidases. Once the hydrogen is removed an unstable compound is formed, which then spontaneously decomposes to form the desired OH. Oxidative dealkylation is a very common metabolic pathway and can either help with the development of a drug or hinder it.
(3) The other atoms are anything but irrelevant. Although most/all of a pharmacophore is essential to elicit a biological response, the rest of the molecule determines how well it binds to the target, as well as physical and pharmacokinetic properties, toxicity, etc.
(4) This may sound callous, but I don't care. If people are taking very large doses (potentially deadly) of tramadol solely for the purpose of getting high, and this is in any way impacting the ability of a legitimate pain patient to get what is normally a non-addictive drug, then it's too damn bad. You don't take away one of the very few (barely) decent weapons we have in our pathetic pain arsenal because some people might intentionally abuse it, despite the prevailing attitudes at the CDC and DEA.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


