
I do not know Dr. Andrew Kolodny, personally, and, aside from one brief phone call last year, I have had no contact with him. Therefore I cannot know his motivation for becoming a driving force behind "opioid reform"— a concept which would border on hysterically funny if not for the tragedy that it is causing in this country.
Dr. Kolodny, a psychiatrist, is the executive director of Physicians for Responsible Opioid Prescribing (PROP)—a group that played a significant role in creating the disastrous CDC Guideline for Prescribing Opioids for Chronic Pain (2016). The CDC ended up incorporating many of PROP's recommendations, which were supposedly designed to help the US mitigate the damage done by opioid (1) drugs, despite the fact that the "evidence" contained in the recommendations had been carefully scrutinized and found unsupportable by FDA scientists.
Since I cannot read his mind, I have no way of knowing whether Kolodny's efforts are an honest, but misguided, attempt to help, or something else.
But I can read his writings, and based on "The opioid epidemic in 6 charts," recently published in The Conversation, honesty is not the word that first pops into my mind. Yes, Dr. Kolodny does present 6 charts to explain his version of what I will now call "The Fentanyl Crisis," (2) but even a quick read of his editorial reveals that it appears to be designed to confuse rather than clarify matters. Let's take a look.
Trick #1: Manipulative and misleading statistics.
"Drug overdose deaths, once rare, are now the leading cause of accidental death in the U.S., surpassing peak annual deaths caused by motor vehicle accidents, guns and HIV infection."
This sentence, the very first of the editorial, doesn't pass the sniff test. Why?
- The term "drug overdose deaths" (there are about 60,000 annually) is now standard jargon used to characterize fatalities from all drugs of all sorts, anticoagulants, antidepressants, aspirin, cocaine, etc. But most people will read what Kolodny wrote and arrive at the conclusion that 60,000 people were killed by prescription pain medications. They were not. All opioids together (including heroin) killed 30,000 people. The number of deaths from prescription opioids—the target of the current crusade— was about 17,000— half the number killed by accidental falls. Are we having an "accidental fall epidemic?" Why not? Accidental falls are killing twice as many people as prescription pain medicines.
- The figure 60,000 is, of course, inaccurate, but so is 17,000. This is because opioid overdose deaths are frequently the result of combination with other drugs, especially benzodiazepines, which potentiate the effect of the opioid action. In 2015 almost half (7,500) of the overdose deaths from opioids also involved benzodiazepines (Figure 2). When you include other drugs that are taken with opioids, especially alcohol and cocaine, It can reasonably be assumed that the number of deaths from opioid pills alone will be much lower, perhaps in the neighborhood of 5,000—ten-times lower the 60,000 that Kolodny implies, and roughly the same as bicycle and bicycle-related deaths. This is what the hysteria is about?
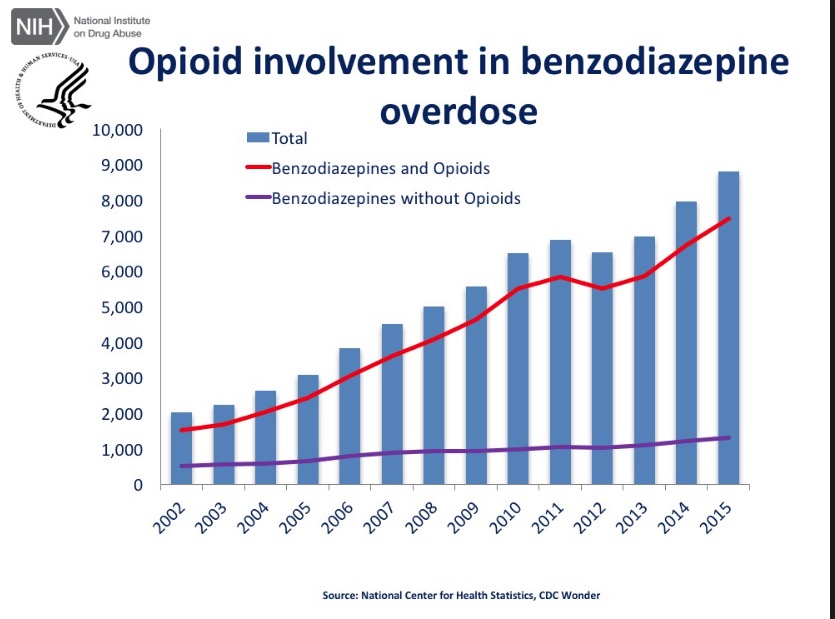
Figure 2. Opioid involvement in benzodiazepine death, And also benzodiazepine involvement in opioid deaths.
- Comparing the number of drug overdose and motor vehicle deaths is pointless, arbitrary and manipulative. What's more, these unrelated numbers can be interpreted in either of two ways. Annual deaths from auto accidents peaked in 1972—before seatbelt laws were in effect—and decreased by 41% as of 2011. What was responsible for the switch? Was it rising drug ODs? Decreasing auto accidents? Both? Does it matter? No, it doesn't. It's a stupid comparison.
- A comparison to deaths from HIV is similarly meaningless. HIV deaths have declined because of antiretroviral drugs.
This same sentence could be rewritten to be just as accurate, but send an entirely different, albeit, still pointless message:
"Life in the US is now significantly safer. The number of annual deaths from automobile accidents, AIDS, and guns is now lower than that from drug overdoses, even when illegal street drugs, such as heroin, are included."
Trick #2: Telling a half-truth.
"The effects of hydrocodone and oxycodone on the brain are indistinguishable from the effects produced by heroin. "
Yes, they are. But Kolodny omits a vital bit of information — potency. While the physiological effect of hydrocodone on the brain may be the same as heroin (the two drugs hit the same receptors), the functional difference between the two drugs is night and day. The magnitude of the effect is conveniently omitted from this "equation." Heroin packs a much more powerful punch than hydrocodone, especially at doses that are used by addicts. People can become addicted to heroin (or even die) from a single injection. It is virtually impossible for one hydrocodone pill to kill or addict anyone. The two drugs don't even belong in the same sentence, even though they happen to belong to the same class of drugs.
Trick #3: The absence of evidence is not the evidence of absence.
"In cases [of long-term use], opioids are more likely to harm patients than help them because the risks of long-term use, such as addiction, outweigh potential benefit. Opioids have not been proven effective for daily, long-term use."
- Trick #3 actually consists of a trick and maybe even a lie. Opioids may not have been proven to be effective for long-term use, but this is because such studies have not been done. This does not mean that opioids have been proven ineffective, even though the wording of this sentence implies this.
- The "lie" about addiction potential of opiates is perfectly obvious to anyone who has read the literature on addiction. The risk of addiction is very low for pain patients (less than 1%) who take pain medicine to control their pain. Overwhelmingly, addiction arises from recreational, not therapeutic use of these drugs.
Trick #4: Blame the drug companies.
"The increase in opioid prescription was fueled by a multifaceted campaign underwritten by pharmaceutical companies. Doctors heard from their professional societies, their hospitals and even from state medical boards that patients were suffering needlessly because of an overblown fear of addiction."
- This tactic is appallingly unoriginal. There is no better way to shore up a weak argument than to introduce an "enemy." And if there is one failsafe enemy, it is the pharmaceutical industry. There is little doubt that there was malfeasance taking place, especially involving companies that were pushing the idea that certain drugs were safer than they really were. Purdue, the makers of OxyContin was fined $653 million for its former actions. Other companies are now being investigated. But this is now irrelevant. Assigning blame may score some points with the readers, and provide fodder for trial attorneys, but does absolutely nothing to keep a single OD victim alive. Whatever certain companies did two decades ago is partly responsible for starting today's fentanyl OD epidemic, but it has nothing whatsoever to do with keeping it going.
Trick #5: Twist the truth
"Why did this happen? A common misconception is that so-called “drug abusers” suddenly switched from prescription opioids to heroin due to a federal government “crackdown” on painkillers. There is a kernel of truth in this narrative."
Yes, there is, barely. But it is only a small part of the story. What Kolodny cites as a common misconception is probably a result of his twisting what I have written in previous articles (See: No, Vicodin Is Not The Real Killer In The Opioid Crisis and Heads In The Sand — The Real Cause Of Today's Opioid Deaths). Except I never said this. The reasons for opioid abuse are multifactorial, but there is no question that epidemic began to escalate in 2010, not from any crackdown, but from an improvement in the formulation of abuse-resistant OxyContin and the unintended consequences that followed. This is indisputable:
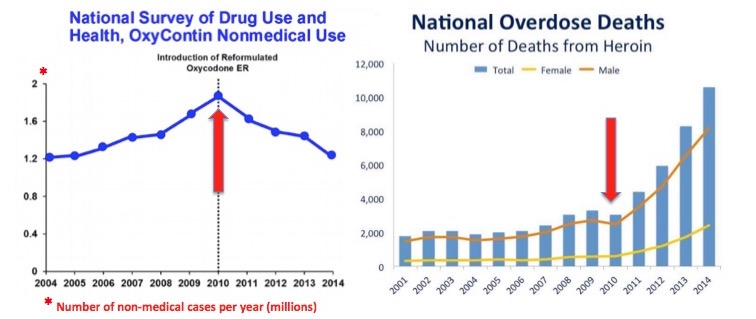
From this point on, there was a "shortage" of pills, both because of market forces and government intervention. The difficulty in getting pills was clearly responsible for some/most of the switch to heroin. Koldony's statement itself was a "kernel of truth." And a rather small kernel at that.
Now let's look at what is really going on. Figure 3 makes this crystal clear. Despite seven years of increasing "vigilance," the number of deaths caused by prescription pain medications remains unchanged, yet total opioid overdose deaths have increased dramatically. The reason is obvious. Virtually all of the additional overdose deaths since can be accounted for by increased use of heroin/fentanyl. Prescription pain medicines are much more difficult to get than 7 years ago, and the only result has been suffering by pain patients and no benefit. It could be no other way. Pills are not the primary driver of overdose deaths. They never were. 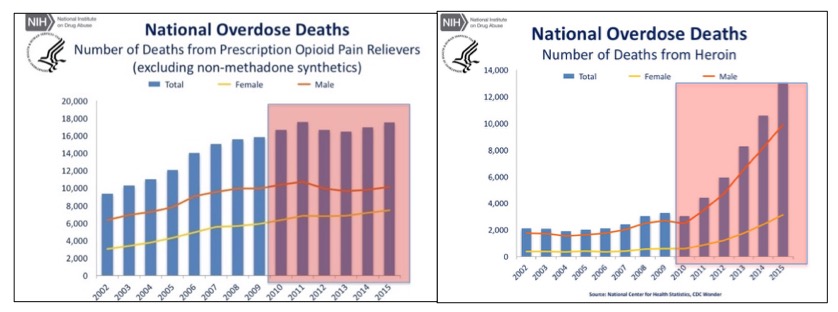
Figure 3. The futility of limiting prescription pain medication. The result was more deaths from heroin/fentanyl and nothing else.
Trick #6: Ignore what doctors are saying.
"Here’s another reason not to believe the narrative about a “crackdown” on painkillers leading to a sudden shift to heroin: There hasn’t been a crackdown on prescription opioids."
To say that there hasn't been a crackdown on opioid prescriptions is to ignore reality. Pharmacy chains are imposing bureaucratic barriers on filling prescriptions and denying prescription refills. The US Association of Attorney's General is lobbying US Insurance providers to revise their formularies to emphasize non-opioid medications in preference to opioids. The Veterans Administration has been directed by Congress to make the CDC prescription guidelines mandatory rather than voluntary. Hospitals and pain management practices all across America are discharging patients and forcibly tapering down the dose levels of those they retain.
And Kolodny's statement also contradicts what every single physician I have spoken with has said. (See: Pain In The Time Of Opioid Denial: An Interview With Aric Hausknecht, M.D.). I'm not sure what Kolodny means by "crackdown," but when doctors are receiving "friendly" warning letters from departments of health and law enforcement agencies, that's not merely a crackdown. It's Kristallnacht.
In closing, although I have questioned whether the intentions of Kolodny and his acolytes are well-meaning or not, it really doesn't matter to the six million people who are cut off from pain treatment in this country. The resulting "opioid pain refugee crisis" is a national disgrace. As is the undue influence granted to a handful of ideologues, well intended or not. As public policy goes, this may be as cruel as it gets.
Notes:
(1) The term "opioids" is scientifically meaningless. Technically, "opioid" means a drug that interacts with the same receptors as morphine, etc., regardless of whether the drug is derived from a natural source, for example, poppy. Opiates are a subset of opioids; they are drugs that are found in plants (e.g., codeine) or semi-synthetic derivatives of them. Heroin, which does not occur naturally, is considered to be an opiate because it is made from morphine, which does. Fentanyl is considered to be an "opioid" because it is not an opium derivative. These classifications are a distinction without a difference. The term "opiates" is more than sufficient to describe drugs with morphine-like properties. The word "opioid" should be dropped from the English language.
(2) There is no such thing as an opioid crisis. It is a fabricated term. People who are now dying from overdoses are now (most of the time) dying from fentanyl and its chemical cousins. A far better and more accurate term is "the fentanyl crisis."

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


