The late politician and sociologist Daniel Patrick Moynihan coined the phrase "defining deviancy down" to describe the tendency of societies to respond to destructive behaviors by lowering standards for what is permissible. Texas physician Dr. Yakov Gizersky described a lamentable example of this in a letter to the Wall Street Journal, expressing his surprise at the influence of Diversity, Equity, and Inclusion (DEI) initiatives on medical school admissions.
He related that he had recently become aware of how “politicized the selection and training of …future physicians has become” while his son was applying to medical schools. Dr. Gizersky described his epiphany thusly:
Nearly all the schools requested multiple essays providing a detailed explanation of the applicant’s dedication to DEI and participating in DEI-related activism. Some schools had essays querying the applicant’s activism for or opinion of progressive border policies. Most also requested that students discuss how they have been adversely affected by systematic racism (and if they haven’t been affected, then they should discuss what they plan to do to fight systemic racism, anyway).
Finally, he noted that some medical schools have stopped requiring applicants to take the Medical College Admission Test, a useful predictor of medical school performance, for “specific applicant groups.” (Emphasis added.)
Dr. Gizerky’s observations took me back… When I entered medical school at the University of California, San Diego, in the 1970s, a requirement for graduation was passing both parts of the medical board exams, the "med boards." Part One tested knowledge of basic science; Part Two, clinical medicine. For several years, the medical school had conducted an aggressive program of recruiting and admitting under-qualified minority students. It turned out that they could scrape by on Part One, but many were failing Part Two.
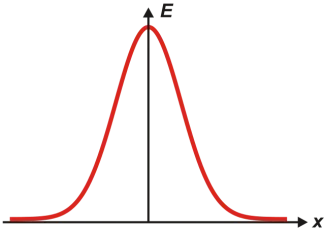
That was not a surprise to my classmates and me. Grades on exams were posted not by students' names but as curves. Ordinarily, you would expect the grades to fall in what's called a "standard normal distribution," or “bell-shaped curve,” that looks something like this:

Instead, the distribution was often more like this:

That implied, correctly, that there were two distinct populations represented by the scores, and we quickly ascertained that the lower distribution consisted of the under-qualified minority students.
Instead of tightening the admissions criteria, the administration responded by lowering the graduation requirement to passing Part One and just taking, but not necessarily passing, Part Two. Nary, a peep was heard from the faculty about this lowering of standards.
This sort of social engineering at medical schools has not been uncommon. Stanley Goldfarb, M.D., a retired dean for curriculum and co-director of the renal division at the University of Pennsylvania's medical school, has repeatedly criticized the trend toward allowing "social justice" considerations to play a dominant role in medical schools' admissions and curricula. He founded a nonprofit called Do No Harm, which aims "to combat discriminatory practices in medicine."
Dr. Gizersky ended his letter to the editor with this observation: “Medical students are already faced with learning more information than ever, and we can’t afford to have medical schools produce better activists than physicians.” I agree, but I would put it somewhat differently: When you're admitted to the hospital for complicated cardiac or neurosurgery, do you want it to be done by the most competent and accomplished surgeon or by one who was admitted to medical school and residency because he or she was a member of an underrepresented group?

Henry I. Miller, MS, MD
Henry I. Miller, MS, MD, is the Glenn Swogger Distinguished Fellow at the American Council on Science and Health. His research focuses on public policy toward science, technology, and medicine, encompassing a number of areas, including pharmaceutical development, genetic engineering, models for regulatory reform, precision medicine, and the emergence of new viral diseases. Dr. Miller served for fifteen years at the US Food and Drug Administration (FDA) in a number of posts, including as the founding director of the Office of Biotechnology.


