Imagine spending a decade of your life dedicated to a malignant, fanatical cause only to have it unceremoniously crammed into the paper shredder by your successors.
Under normal circumstances, one might feel some empathy for people who reached the pinnacle of their professional lives only to see it crumble before them. But if you're looking for any signs of sympathy for the likes of Andrew Kolodny, Jane Ballantyne, and the rest of the anti-opioid zealots who destroyed so many lives in such a short time, it will be like hunting for glaciers in the Sahara.
I doubt that "opioid phobia" will be vanishing anytime soon, but it took a big hit today when the CDC released its long-awaited draft revision of its 2016 opioid prescribing guideline – a 221-page slap in the face to Physicians for Responsible Opioid Prescribing (PROP), which I renamed Physicians Responsible for Opioid Prohibition. I can think of no better name for the sinister group of dilettante academics that somehow insinuated its way (1) into a process of establishing unprecedented, cruel, medically unsound, and probably unconstitutional policies that devastated millions of chronic pain patients.
Perhaps they are experiencing some well-deserved karmic pain of their own. That's OK; they're earned. I plead guilty to schadenfreude.
Although the draft document that blows up the 2016 CDC/PROP abomination isn't perfect, upon first inspection, it's pretty damn good. Let's take a look at a few of the highlights.
From the introduction alone, we can immediately see a shift from "let's treat pain patients like addicts and get them off these horrible drugs."
This clinical practice guideline is
A clinical tool to improve communication between clinicians and patients and empower them to make informed, person-centered decisions related to pain care together...Intended to be flexible to enable person-centered decision-making, taking into account an individual’s expected health outcomes and well-being.
And...
This clinical practice guideline is not
A replacement for clinical judgment or individualized, person-centered care...Intended to be applied as inflexible standards of care across patients, and/or patient populations by healthcare professionals, health systems, pharmacies, third-party payers, or governmental jurisdictions or to lead to the rapid tapering or discontinuation of opioids for patients
In other words, a complete and total repudiation of laws and policies of the past six years. Some examples:
- 2016: Hard limits, based on a flawed MME table, became law in 36 states. These limits governed patient care.
- 2022: Doctors and their patients, not the government, will together decide on the protocol for pain care.
- 2016: All pain patients are treated the same.
- 2022: Flexible treatment based on the needs of individual patients.
And, perhaps most important:
- 2016: "Advice" somehow led to the barbaric practice of forced tapering.
- 2022: No rapid tapering or discontinuation of opioids for patients.
Some other highlights include:
It is imperative that people with pain receive the most appropriate and effective pain treatment with careful consideration of the benefits and risks of all treatment options.
This could not be more different than what's happening today. The maniacal drive to get pain patients off opioids resulted in the use of more dangerous and/or useless drugs (e.g., high dose NSAIDs and Tylenol) and off-label, experimental, and probably useless drugs (e.g., antidepressants, gabapentin, marijuana, and other cannabinoids), as well as questionable non-pharmacological methods (e.g., acupuncture, yoga, cognitive behavior therapy, music therapy).
Don't get me wrong. I'm not saying that there is any reason not to try non-opioid methods of pain control. If they work, fine, But the hundreds of pain patients that have written to me consider most of these techniques to be a bad joke. Playing Mozart for someone with a crushed spine isn't going to cut it.
Clinicians should avoid abrupt discontinuation of opioids, especially for patients receiving high dosages of opioids, should avoid dismissing patients from care...
Although this sounds like a huge improvement, it is probably too late to reset. Afraid of DEA persecution, most pain management physicians have left the field entirely. In theory, avoiding dismissing patients from pain sounds both humane and logical, but this has already happened. It is challenging to find a pain patient who still has a pain management physician to treat them, let alone one who hasn't involuntarily cut their dose. I don't know how this gets fixed.
It's Good, But Not Perfect
1. The MME measurement remains
Although the passage below is clearly intended as a guide rather than a mandate, it is nonetheless disturbing to see the term used at all, something I wrote about in 2018: "The use of the Milligram Morphine Equivalents is scientifically flawed because it fails to take into account even the most basic tenets of pharmacology, rendering it scientifically meaningless."
Many patients do not experience benefit in pain or function from increasing opioid dosages to ≥50 MME/day but are exposed to progressive increases in risk as dosage increases. Therefore, before increasing total opioid dosage to ≥50 MME/day, clinicians should pause and carefully reassess evidence of individual benefits and risks.
2. So does the MME conversion table
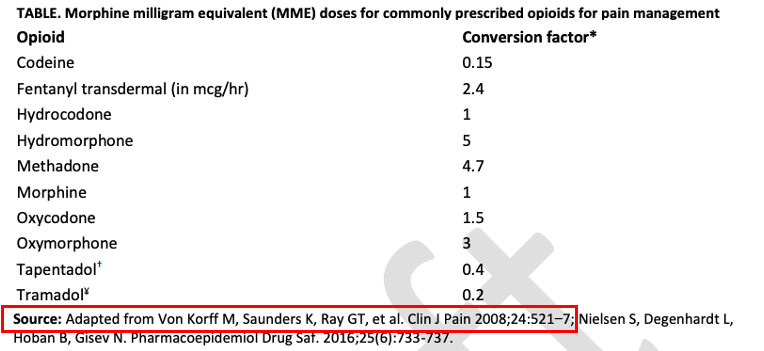
This table is rather troubling:
- This table is, at least in part, derived (red box) from a 2008 paper by Von Korff (a co-founder of PROP). The 2008 paper proposes a similar conversion table, but it is based on a collection of small, single-dose studies – a shortcoming recently described by Dasgupta and colleagues in The Clinical Journal of Pain [emphasis mine]:
Contrary to conventional wisdom, conversion values are not based on pharmacologic properties. Instead, they arose 60 years ago from small single-dose clinical studies in postoperative or cancer populations with pain score outcomes; toxicologic effects (eg, respiratory depression) were not evaluated.
Nabarun Dasgupta, et. al., The Clinical Journal of Pain: August 2021 - Volume 37 - Issue 8 - p 565-574 doi: 10.1097/AJP.0000000000000948
Bottom line
It is not trivial to condense 221 pages into one article; there is much more to write about. But I was pleasantly surprised to see the revised guidelines. Although some of them may be difficult to implement, and there remain some troubling remnants of the 2016 document, I give the CDC a thumbs up.
Note:
(1) How did Andrew Kolodny become the national spokesperson on opioid policy? Ask Tom Frieden, the former director of the CDC from 2009-17, precisely when the Guidelines were being formulated. The connection? See Pat Anson's article about the connection between the two.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


