
Senator Susan Collins (R‑ME) wrote an op‐ed for Seacoastonline this week expressing her concerns about skyrocketing drug overdose deaths. According to the most recent data from the National Center for Health Statistics, 90 percent of opioid‐related overdose deaths involve illicit fentanyl, and 15 percent involve diverted prescription pain pills. In her column, Senator Collins expressed pride in a proposal aimed at reducing overdoses that she co‐sponsored with Senator Michael Bennet (D‑CO). Unfortunately, while the legislation was well‐intended, it placed too much emphasis on educating doctors to curtail opioid prescribing to their patients in pain and not enough on the root cause of the surge in fentanyl‐related deaths: the “iron law of prohibition.”
Though their legislation laudably eliminated the requirement that doctors who treat addiction with buprenorphine go through the onerous process of obtaining a special “X” waiver from the Drug Enforcement Administration, it placed a new burden on all doctors who treat pain: they must take an 8‑hour course in opioid prescribing for pain that is approved by the DEA in order to maintain their narcotics prescribing license. The American Medical Association correctly opposed this provision arguing that more than 40 states already require physicians to take similar courses, the courses have not reduced overdose deaths, and the added burden is likely to make some doctors quit prescribing narcotics altogether, further reducing pain patients’ ability to get relief.
Senators Collins and colleagues remain fixated on the discredited idea that the overdose crisis was caused by doctors overprescribing pain medication to their patients. But as I have written numerous times, data from the Centers for Disease Control and Prevention (CDC) and the Substance Abuse and Mental Health Services Administration (SAMHSA) reveal there is no correlation between prescription pain pill volume and non‐medical use or addiction to prescription pain pills. Furthermore, researchers at the CDC and the University of Pittsburgh School of Public Health reported in 2018 that overdose deaths have been rising exponentially since at least the late 1970s, with different drugs being in vogue and predominating among the overdoses at various points in time.
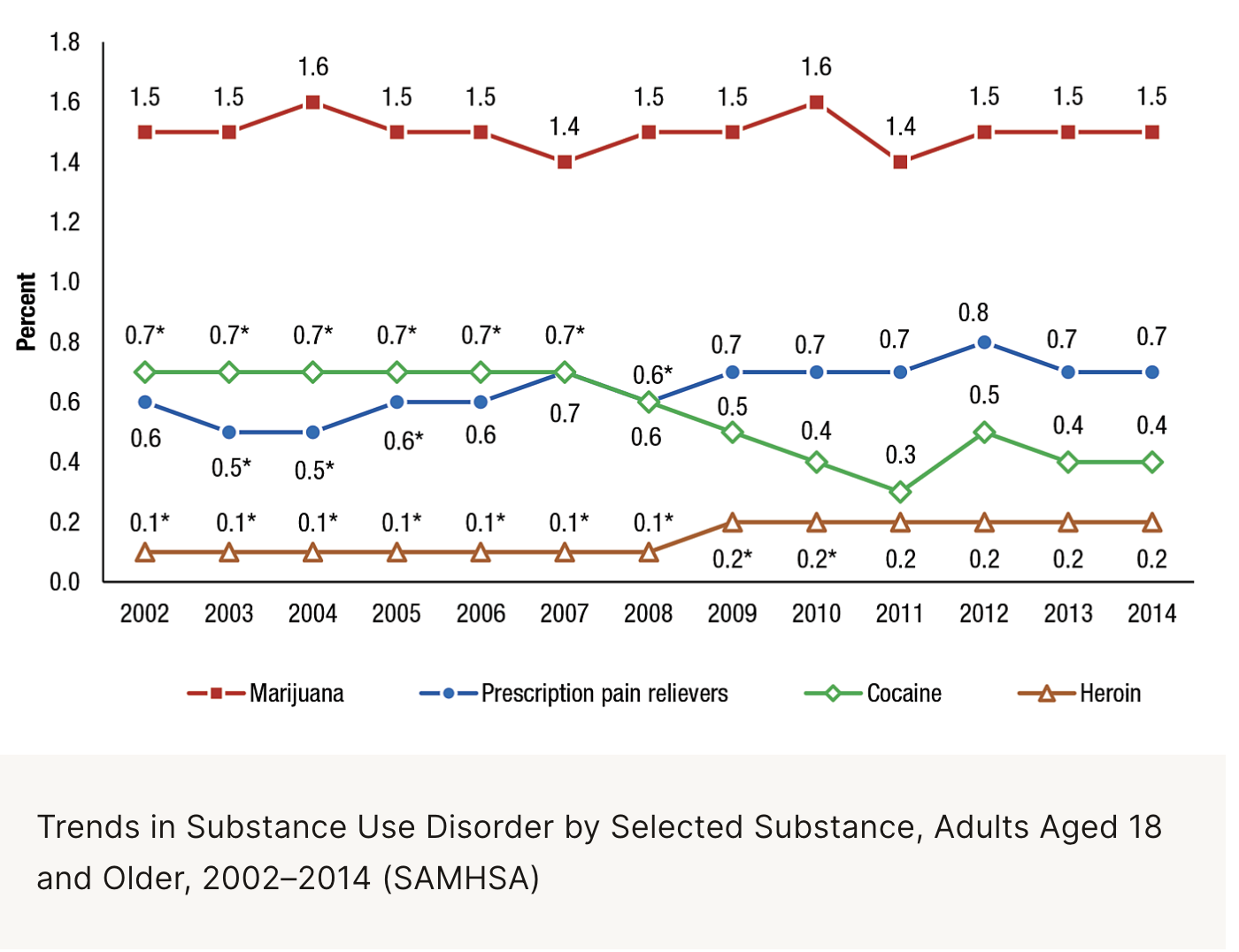
The National Survey on Drug Use and Health, conducted by SAMHSA since 2002, reveals that the addiction rate for persons over age 18 has been essentially stable at less than 1 percent since the year the survey began (see attached graph from SAMHSA). That finding is incompatible with the false narrative that doctors created a population of zombie‐like opioid addicts by overprescribing pain pills.
A study by researchers at Harvard and Johns Hopkins published in the BMJ in 2018 followed over half a million patients treated with opioids for acute postoperative pain from 2008–2016. The researchers found a total misuse rate of 0.6%
A study released this week in the Yale Law and Policy Review revealed that only 9 percent of non-medical opioid users in 2001 reported ever using OxyContin (made by Purdue Pharma) during their lifetime. It found that codeine, often mixed with soft drinks, was responsible for much of the spike in non-medical opioid use in the 1990s.
The CDC reports that at least 80 percent of overdose deaths are polydrug, i.e., they involve combinations of multiple drugs. Non‐medical users often combine opioids with stimulants like methamphetamine and cocaine, or tranquilizers such as Xanax or alcohol. The New York City Department of Health reported that 97 percent of overdose deaths were polydrug as early as 2015.
A 2019 study in North Carolina found at least three‐quarters of NC opioid‐related overdose deaths involved cocaine, meth, and alcohol.
If the opioid overdose deaths were due to overprescribing opioids, the toxicology studies would only contain opioids. Doctors are not prescribing polydrug cocktails; we’re not recommending opioids plus cocaine plus meth plus alcohol to our patients. And why would dependence on opioids compel a person to use them with cocaine, meth, Xanax, and alcohol?
Senator Collins and her congressional colleagues should drop their obsession with doctors treating pain patients and acknowledge that the overdose crisis has always resulted from drug prohibition and the inevitable black market that results, filled with dangerous and increasingly potent products. Ideally, they should end America’s longest war—the war on drugs. Short of that, they should at a minimum, shift their focus away from doctors and patients and toward meaningful harm reduction. A chapter in the 9th edition of the Cato Handbook for Policymakers points the way.
By continuing to focus on doctors and patients, Senator Collins and her colleagues are still fighting the last war and against the wrong targets.
#Reprinted with permission. Dr. Singer's original blog post can be read on the Cato Institute site.



