
Here's a first. A study that might actually disprove itself. I've never seen anything like it.
A paper in JAMA Open Network tries to hop on the anti-opioid bandwagon but fails so badly that I had to stare at the screen in disbelief for a while. Did I really just see this? Does it mean what I think it does? Did the authors fail to realize what their own data say?
Here's the title:

The intent of the study is obvious - to let us know that more pharmaceutical money leads to more opioid prescriptions being written, which results in more OD deaths. While this may be "intuitively obvious," this does not make it correct. Here's why.
The authors, mainly from Boston Medical Center, gathered prescription data from 67,507 US physicians in 2,208 counties between August 1, 2013, and December 31, 2015. They used these data to assert (Cue to "Same Old Song," Four Tops, 1966) that the more that drug companies push opioid pills to doctors the more people died over a 2+ year period. But they may have given us cause to reach an entirely different conclusion.
Let's start with their Table 2, which examines the association between pharma money and OD death using three different models, each of them representing a different way of measuring "money."
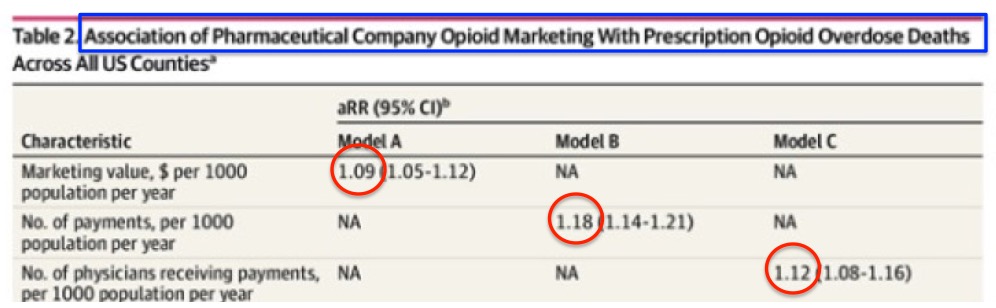
Table 2 (partial): Source: JAMA Network
There are three ways that the scientists used to measure pharma money: marketing dollars (A), the number of physician payments (B), and the number of physicians who received payments (C). In each model, there is an associated relative risk (RR) of increased deaths in those counties ranging from 1.09-1.18, which means a 9-18% increase.
ACSH advisor and expert biostatistician Dr. Stan Young is uncharacteristically understated:
"An odds ratio, OR, of 1.000 is even odds, no effect. If an OR is close to 1.000, then any small bias could have produced the effect. An OR of 1.1 is not impressive."
Dr. Stan Young, private communication, 1/23/19
In other words, when the increased relative risk is so low the presence of any kind of bias, for example, age, race, socioeconomic status, or the presence of other drugs, could turn the very low observed increase could turn into a zero increase. Even if we assume a perfect selection process, we are looking at an increase in deaths of about 15% at best. In other words, not much.
Now let's look at Table 3, which shows that more pharma money results in doctors writing more prescriptions - something that can't be a huge surprise.
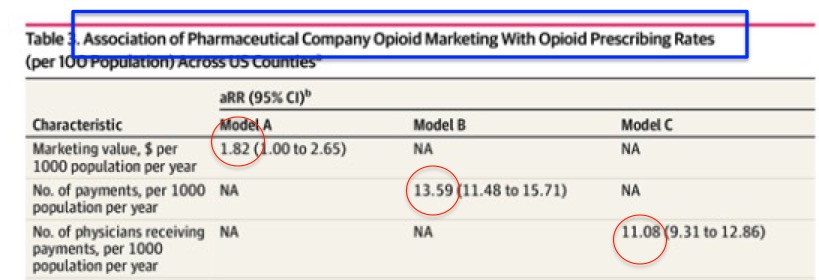
Table 3 (partial): Source: JAMA Network
But now we see that pharma money results in a large increase in the number of prescriptions written by doctors. With a higher relative risk (1.8-13.6-fold, 80-1260 % increase) the chance of bias affecting the results is quite low.
So, let's put these two conclusions together:
A. More pharma money leads to a very small (perhaps, zero) increase in overdose deaths.
B. More pharma money leads to a significant increase in written prescriptions.
So, it is reasonable to conclude that:
C. Despite a whole lot more written prescriptions, the rise in OD deaths is minimal, if any.
So, it's also reasonable to conclude that:
D. Prescribed opioids aren't causing many (or any) deaths, something that patient advocates have been screaming forever.
There are other limitations of the study that are disclosed in the paper as required. It would be rather easy to debunk the study based on these alone. But let's not. Instead, let's ask a question: Did the authors start out trying make a point only to end up making the opposite point instead? If so, do they realize this? Or are they just hoping that we don't?
I have no idea. Perhaps someone can explain? Crazy.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.

