Does the media have it right, did a new study show that drinking 2 or more artificially sweetened beverages a day result in a greater risk of stroke? I don’t think so, but here is the information, you decide.
Comparing apples and oranges
This was a study of the “observational wing” of the longitudinal Women’s Health Initiative which recruited participants in the mid-’90s. Participants were asked to estimate this use of artificially sweetened beverages (ASB) 3 years after enrollment and the study reports how they fared since that report. While consumption was initially gathered into nine categories, two-thirds of the women did not drink any ASB at all or rarely, and to achieve reasonable sample size the groups were collapsed into 4, that >2 ASBs/daily included those drinking up to and more than six a day. The reported figures further collapsed the data to compare essentially no ASB consumption to>2 per day.
These participants with that >2/day habit differed in other ways from the abstainers. Specifically, they were more likely overweight or obese, poorer diets with more calories in, less exercise, more current or prior smokers, with higher incomes and educational levels. Oh yes, they were more likely to have histories of diabetes, myocardial infarctions, or strokes. The report points out that the majority of these ladies never or rarely drank “regular” soda, but twice as many of them did drink regular soda compared to the abstainers.
The results
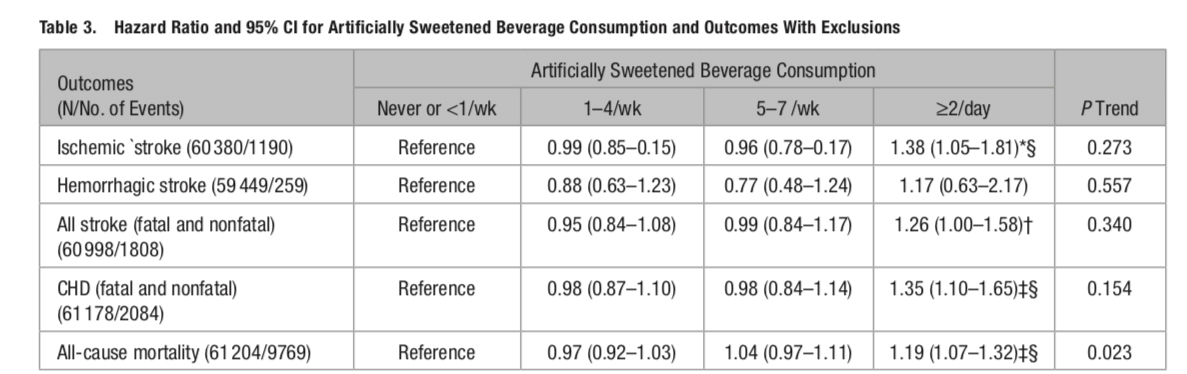
This was the data when they excluded women who already had diabetes or cardiovascular disease. The § indicates a statistically significant value when comparing the highest to the lowest. But look at the p values for the trend, not a significant value in the bunch. The authors do explain, “It is important to note that where P for trend is not significant, but the highest category of ASB is significantly different from the lowest, we may be observing an association that has a threshold or other nonlinear relationship.”
A deeper dive into the ischemic stroke data shows that ASBs were associated with only small vessel strokes, one of the three subtypes, representing about one-third of the strokes. The other subtypes, strokes due to carotid artery disease or embolism from the heart, had no statistically elevated risk, in fact, for carotid disease, ASBs were protective reducing strokes by 74% (if you believe statistics).
While the study participants were mostly white, the study’s most robust findings were in the 7% of black participants. Here are the authors, “Higher ASB consumption was significantly associated with higher ischemic stroke risk among blacks (HR 3.93 …) but not among whites or other race/ethnic groups.”
The authors acknowledge that it was an observational study, and the characterization of ASB consumption was hampered by it being self-reported a median of 11 years previously and that it did not necessarily include ASBs used in coffee or tea, or which artificial sweetener was consumed.
My takeaway is that the variable of interest is poorly characterized, aggregated to the point that a statistical significance was identified. The ASB consumption was a fellow traveler with obesity, less exercise, more calories, poorer food choices; so why are they not the real risk factors? The actual finding was a racial distinction; black women had more strokes, white women more cardiac events – and ASBs along with the being overweight, under-exercised, and eating a less nutritious diet makes those events more common. And none of this applies to men, or women below the age of 50, the other 85% of the population.
The media reports are wrong because they are incomplete. The headlines capture eyes, the text, painted too broadly, reinforces a cultural narrative rather than providing a nuanced scientific understanding. That’s the thing about “fake” news, it has an element of truth but is wrapped in a context that misleads and confuses.
Source: Artificially Sweetened Beverages and Stroke, Coronary Heart Disease, and All-Cause Mortality in the Women’s Health Initiative Stroke DOI: 10.1161/STROKEAHA.118.023100

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


