
“… there is a strong scientific rationale and evidence that viruses are very efficiently spread through aerosols by the patient's breathing only. It is not necessary for the patient to cough or sneeze. The exhaled aerosol particles are generated by normal breathing in the deep lung … [and can be] present in the room air for hours. …These aerosol particles are difficult to filter out of the air; because of their physical properties.”
These are the words of Dr. Gerhard Scheuch, writing in the Journal of Aerosol Medicine and Pulmonary Drug Delivery. His review suggests that simply the act of breathing, not coughing or sneezing, is the source of aerosols containing airborne pathogens, including COVID-19. It falls to each of us to clean up our breath.
If we are infected, we need to breathe in clean air and exhale a scrubbed breath, free as possible, of viral particles. The problem, of course, is that we are transmitting the virus for days before we become symptomatic if we become symptomatic at all.
Mask Up
If we are healthy, no harm, no foul, perhaps some inconvenience. But if we are sick with COVID-19
then, you and I may be causing bodily injury or even contributing to the premature death of our fellow citizens.
Some say masks don’t work. They have arguments, some based on scientific research done before the current pandemic and a single randomized control trial in Denmark where mask use seemed to be inconclusive or could be shown to be making little difference.
Can we trust the masks that we are asked to wear?
Here is what I found when I looked at this question. [1]
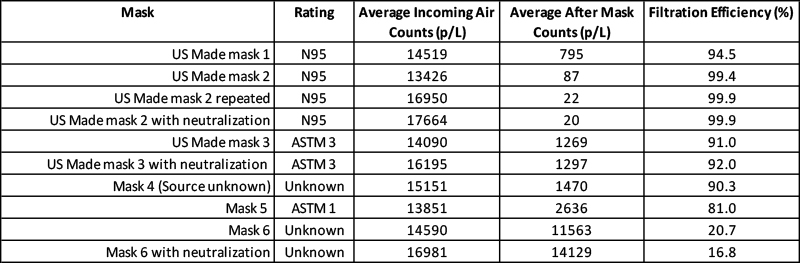
The data shown in the table are from work in progress. It is an experiment to measure mask filtration efficiency using normal room air. Our system measures filtration effectiveness in the size range associated with the virus identified as COVID-19 and its variants. The masks we tested are suitable for clinical use, around infected patients, with tests showing greater than 95% filtration efficiency for bacteria and test particles and good breathability and resistance to liquid penetration. Products meeting these standards are worthy of your confidence, and all are readily available – several of the above were purchased on Amazon.
You might note that several masks tested reference the phrase “with neutralization.” The aerosols we exhale may be electrically charged (think static electricity from movement). Standardized testing of masks that use salt aerosols often will include a “neutralizing” variable where the test aerosols have been changed to have a uniform or standard ionic charge.
All of the masks effectively filtered room air, some more than others, but the bottom line is that an easily purchased mask can reduce your exposure and possible transmission of COVID-19 sized particles. These mask works as well in healthy individuals, as those with COVID-19, vaccinated or not.
What is the takeaway here?
We must find a way to decrease the health risk from the virus emitted by others, and give others, the benefit of a reduction in risk from the virus we may be emitting. This is not political and has little to do with freedom. It is the applied practice of environmental medicine and the essence of public health and prevention. It follows the Golden Rule, “Do unto others as you would have them do unto you.”
[1] You can find a short explanation of the methodology used in my previous article.
Special thanks to my colleagues Dritan Xhillari and Ryan Archer for their help in this work



