
The FDA continues to ponder whether mixing two types of vaccines may improve their efficacy. Some reports are beginning to hit the literature; here is a report from Sweden published in the Lancet.
The AstraZeneca vaccine was the most widely used in Sweden, although many received either of the two mRNA vaccines. The data from the Swedish Vaccination Register – physicians are mandated to report vaccinations, so this information covers everyone in the population. All individuals had received one dose of the AstraZeneca vaccine; many received a second dose – homologous vaccination. Two additional groups were identified receiving the second dose of one of the mRNA vaccines – heterologous vaccination.
The study identified 430,000 people receiving homologous vaccination and matched them with 110,000 unvaccinated controls. This cohort was slightly older at 67 than the “mixed” use group at 44. One must consider that the susceptibility of these age groups favors the mixed case. A total of 94,000 people received Pfizer as their second dose, 16,000 received Moderna, again with matched unvaccinated controls. Hypertension and diabetes were the more common co-morbidities. The mean follow-up was just shy of 3 months.
The findings
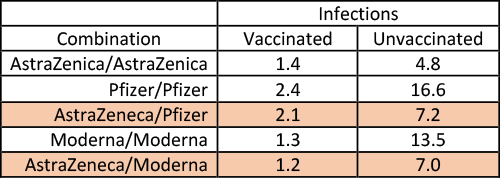 The values are the cases/100,000
The values are the cases/100,000
person-days. The denominator is the product of the number of participants x the days since their vaccinations. I have used color to highlight the differing effects of the Moderna and Pfizer second doses compared to their homologous use. Over two months, there were a total of 19 hospitalizations, 16 among the unvaccinated, two having had two AstraZeneca doses, one a second dose of Pfizer’s vaccine.
- Vaccination, whether mixed or matched, was significantly more protective than no vaccination at all.
- The Pfizer vaccine seemed slightly less effective than AstraZeneca or Moderna. (But again, the dosages of these three vaccines vary.) These findings have varied with different populations, so we might assume it may not be as generally applicable to all folks.
- Mixing was associated with a slightly better response than matching. There is clearly no downside to mixing, and there may be a benefit.
A preliminary report from the US, shared with the FDA, also suggests that mixing may heighten the immune response. In this much smaller study of 450 individuals, the mix was between the two mRNA vaccines and the J&J vaccine. A matched J&J booster increased antibody levels 4-fold, Moderna increased the levels 76 fold, and Pfizer increased about 35-fold. It is essential to recognize that the outcome here was a change in antibody response, a less direct marker of protection than infections themselves, the effect of interest in the Swedish report.
Even with that caveat, there does seem to be credible evidence that mixing may offer some advantages. There is one other piece of observational, although more anecdotal evidence, we might consider. Those individuals who have recovered from COVID-19 and subsequently vaccinated with an mRNA vaccine seem to do best of all. Again, no one is suggesting that this is the best or even reasonable path forward.
To reiterate another important distinction, we need to consider both our immune response's strength and broadness. Antibody levels are a reasonable measure of strength, as our T cell counts. But both fail to describe which component of the virion is considered foreign and being “attacked.” We know that the mRNA vaccines are specifically targeted against portions of the spike protein. The J&J product may not be as specific. Recovery from a COVID-19 infection seems to cover more areas on the virion than just a focal area of the spike.
Mixing vaccines were initially introduced as a measure when vaccines were scarce; production was not fully ramped up. The new data may provide a new approach. It will undoubtedly take more time to gather sufficient data on the response of a US population to mixed vaccination. But the time frame for deciding may rest more with the virus than with our scientists and regulators. We might have to settle with uncertain data – at the moment, the observational data says it can’t hurt and may help.
Source: Effectiveness of heterologous ChAdOx1 nCoV-19 and mRNA prime-boost vaccination against symptomatic Covid-19 infection in Sweden: A nationwide cohort study Lancet Regional Health DOI: 10.1016/j.lanepe.2021.100249

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


