
“Hall and his colleagues did their best to ensure that the only significant difference between the two groups was in how much processed food they consumed. Each group ate diets that were nutritionally identical in every way Hall and his team could think of, containing the same amounts of sugar, salt, fat, fiber, macronutrients, carbohydrates and calories. …
Hall, it turns out, had it all wrong—processing, in fact, made all the difference. …The conclusion: whatever food company chemists are doing to food, it makes people fatter.”
Ultra-processed foods are “formulations mostly of cheap industrial sources of dietary energy and nutrients plus addictive, using a series of processes.” That said, they are
- Inexpensive
- Have a long shelf-life
- Are relatively safe from the microbiological perspective
- Provide important nutrients
- Are highly convenient
- High in calories, sugar and fat “and have been suggested to be engineered to have supranormal appetitive properties.” [emphasis added]
The experiment performed by Dr. Hall and described in the Newsweek article was designed to consider the effect of those processed foods on energy intake. The study involved 20 subjects, 10 of each gender, median age 32, BMI in the normal range. Over a 28-day study, they were given three meals a day and snacks. One group received ultra-processed foods, the other unprocessed foods matched for calories, energy density, micronutrients, fiber, sugar, and sodium – to the best degree possible, the diets differed only in one group having been processed differently. After two weeks, the groups switched to the alternative diet. Participants had 60 minutes to eat their meals, and snacks were available throughout the day. All were housed in a metabolic unit at the NIH and exercised to the same degree daily.
We can argue about some of the subtleties of the experimental design, e.g., there was no washout period between the change in diet to return to baseline, but this is a rigorous study and avoids many of the pitfalls of observational studies. I believe the findings to be valid. Here are the findings:
- It cost $106 a week to provide 14,000 ultra-processed calories, $151 for the same amount of unprocessed meals.
- Those participants in the ultra-processed diet took in 500 calories a day more than the participants eating unprocessed meals. And remember, the groups switched diets at mid-point, so this is not a result of different groups of individuals.
- Those extra calories were derived from excess carbohydrates (280 calories) and fats (230 calories), not protein
- Energy intake remained stable with the unprocessed diet and dropped by about 25 calories a day with the ultra-processed diet.
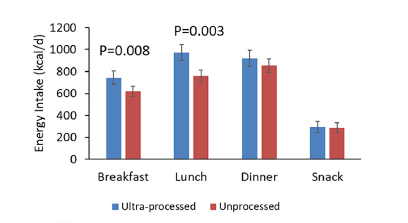
- Those extra calories were eaten as carbohydrates for breakfast and lunch, but not dinner or snacks. Fats were increased for all three meals, but not snacks
- Both diets were rated as pleasant and familiar so that “tasty” was most likely not an issue.
- Those eating the ultra-processed diet gain about two pounds over the two weeks, those eating an unprocessed diet lost the same amount. The weight increase was not associated with their BMIs, but their diet. [I DON'T UNDERSTAND THIS ONE]
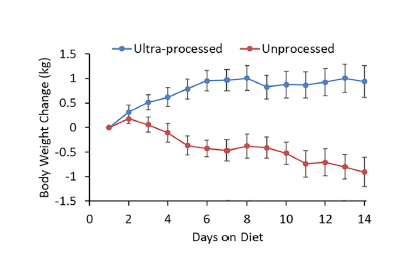 About half that weight gain or loss was in fat-free mass; the researchers thought the remaining changes were due to increased or decreased fat stores and fluid shifts from the differing intake of sodium. The ultra-processed diet had 1800 mg of daily salt, the unprocessed diet 1400 mg
About half that weight gain or loss was in fat-free mass; the researchers thought the remaining changes were due to increased or decreased fat stores and fluid shifts from the differing intake of sodium. The ultra-processed diet had 1800 mg of daily salt, the unprocessed diet 1400 mg- Insulin secretion and blood sugars were slightly greater in the ultra-processed group but were not statistically significant. An oral glucose tolerance test, which stresses the response of insulin to sugar, was the same for both groups
- Across a range of biomarkers like cholesterol and hormones involved in hunger and satiety, there were no significant changes from baseline after eating ultra-processed foods – the researchers ascribed this to ”subjects likely consum[ing] a habitual diet high in ultra-processed foods.” The unprocessed diet did show an increase in an appetite-suppressing hormone, PYY, and a decrease in ghrelin, a hormone signaling hunger.
“Our data suggest that eliminating ultra-processed foods from the diet decreases energy intake and results in weight loss, whereas a diet with a large proportion of ultra-processed foods increases energy intake and leads to weight gain. Whether reformulation of ultra-processed foods could eliminate their deleterious effects while retaining their palatability and convenience is unclear.”
There were no huge differences metabolically. Those eating the ultra-processed diet ate more, and while Dr. Hall took pains to assure the diets were pleasant and familiar, perhaps the ultra-processed diet was tastier. I think instead, they altered our satiety – our feeling of fullness. Consider these findings, also reported in the research, and then we can discuss what makes us feel full and satisfied.
- The energy density, calories per kilogram of food, was higher for the ultra-processed foods – 80% higher. That difference was lower when accounting for the beverages the ultra-processed and unprocessed diets involved, but “beverages have a limited ability to effect [sic] satiety.”
- The ultra-processed diet was also consumed faster, whether measured by consumption in weight or calories.
- The unprocessed diet increased a signal of satiety, PYY, and decreased a signal of hunger, ghrelin.
Could ultra-processed foods alter our feeling of satiety?
While our senses of sight, smell, and taste get us eating what is in front of us, they have little to do with our feeling of hunger or satiety. Satiety is controlled by mechanical, chemical, and central processing or integration of information. The earliest recognized signal of satiety is that “full” feeling we get as our stomach becomes distended with our meal. The presence of a “food baby” is a sure sign we have had enough.
The stomach acts as a reservoir to hold the meal and begin digestion. It has several peptide hormones, each responding to different nutrients that signal satiety to our brain even before the nutrients hit our bloodstream – they act in a sense as a signal that enough nutrients are present for processing by the intestine and that any more would overwhelm the system. As a surgeon, I am most familiar with CCK, which is released in the duodenum, the area between the stomach and small intestine. CCK increases the release of enzymes from the pancreas to digest our food and causes the gall bladder to begin to contract and release bile into our gut to facilitate fat absorption. CCK also signals the brain through the vagus nerve. The response to CCK, which is in isolated experiments, to reduce meal size and is a satiety signal is further increased when the stomach is distended. So, satiety reflects multiple signals. [1]
Adiposity signals are also hormones but are secreted into the bloodstream during meals “in direct proportion to the amount of stored body fat” – a physiologic way of determining how much energy reserve you have. The poster child here is insulin and the lesser-known hormone leptin. While insulin increases in the presence of glucose, its basal level and response to that new glucose are in direct proportion to body fat. Obese individuals “have relatively high basal and stimulated insulin.”
Leptin is directly released from our fat cells, so it is indicative of our energy reserves. Higher levels result in feeling less hungry—rising insulin results in higher leptin levels. In obese people, many have a decreased sensitivity or resistance to both insulin and leptin. This may account for the paradoxical increase in leptin among the obese and among those experiencing emotional stress. The hormonal counterweight to leptin is ghrelin, a product of specialized cells in the GI tract innervated by nerves, neuroendocrine cells. Ghrelin increases your appetite and is highest just before a meal. Bariatric surgery, currently our most effective obesity treatment, can reduce ghrelin levels by up to 60% while also reducing the stomach's capacity as a reservoir of food.
These satiety signals interact directly with our brain, crossing the blood-brain barrier. They are integrated with environmental information, including our eating culture, social situation, and stress levels, producing a “let’s eat” or “that’s enough” response. But here’s the thing, those environmental cues can override all of those satiety signals – the call of “Dessert!!” is a bit of free will behavior, as many of us can attest.
Returning to Dr. Hall’s study, those participants eating the ultra-processed diet ate more quickly; they had a different satiety response, at least temporally. There are a number of ways this can come about, beginning with more calorie-dense foods that have smaller volumes and distend our stomach less. Remember how CCK is more impactful in being a satiety signal when the stomach is distended? As a result, you can take in more calories. Those additional insulin and leptin signals occur later, and if you are overweight, you may be less sensitive to them. Perhaps it is not the nutrients per se or how they are processed or ultra-processed, but how those nutrients alter a more subtle, primitive rhythm of eating. Perhaps that’s why chewing your food longer, slowing down as you eat, and beginning a meal with a calorie sparse soup or salad, results in fewer calories consumed.
Several studies suggest that “obesity is socially infectious” because it is an eating behavior you pick up from those around you, like your family and friends, your network. In one study [2] of 12,000 individuals over 32 years, your chance of becoming obese increased anywhere from 30 to 57% with an obese spouse or friend, respectively. This would also fit in with the idea that “food addiction” is more a behavior addiction than a substance problem.
Obesity has chemical and behavioral components. The Hall study clearly demonstrates that an ultra-processed diet results in weight gain. But all that matching of nutrients and calories in his research may have been for naught; there is equally clear data that an ultra-processed diet is more calorie-dense, that it is consumed faster, and that the combination of those two features throw off our satiety signaling. It means to me that there is no one nutritional culprit and no type of processing that is the smoking gun in our obesity epidemic. Dr. Hall’s paper ends with a final cautionary note in recommending limiting the consumption of ultra-processed foods that we should
“…be sensitive to the time, skill, expense, and effort required to prepare meals from minimally processed foods - resources that are often, in short supply for those who are not members of the upper socioeconomic classes.”
[1] Another of the satiety hormones is GLP-1 glucagon-like peptide-1 which is now used as an injectable medication in treating diabetes. You may know them better as Trulicity or Ozempic, which are not offered as weight loss drugs, but those ads indicate that many people lost 5-6 pounds while on the medication.
[2] The Spread of Obesity in a Large Social Network over 32 Years NEJM DOI:10.1056/NEJMsa066082
Source: Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake Cell Metabolism DOI: 10.1016/j.cmet.2019.05.008
Gastrointestinal Satiety Signals - An overview of gastrointestinal signals that influence food intake American J Physiol Gastrointest Liver Physiol DOI:10.1152/ajpgi.00448.2003.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


