
Academics weigh in
A fear that radiation associated with diagnostic medical care, e.g., X-rays and CT scans, has been taken very seriously. It has spawned a movement demanding that those studies use “As Little As Reasonably Achievable” (ALARA).
In 2009, Rebecca Smith-Bindman, MD, published a research article in the Archives of Internal Medicine, asserting that CT scans posed an alarming danger. She predicted that diagnostic CT scans would cause more than 29,000 major cancers. In succeeding years, she echoed this dire warning often in the media.
“We found that the risk of cancer from a single CT scan could be as high as 1 in 80….”
Bindman derived this alarming prediction from applying a model - the linear no-threshold theory of radiation mutagenesis. Let’s take a moment for a bit of background.
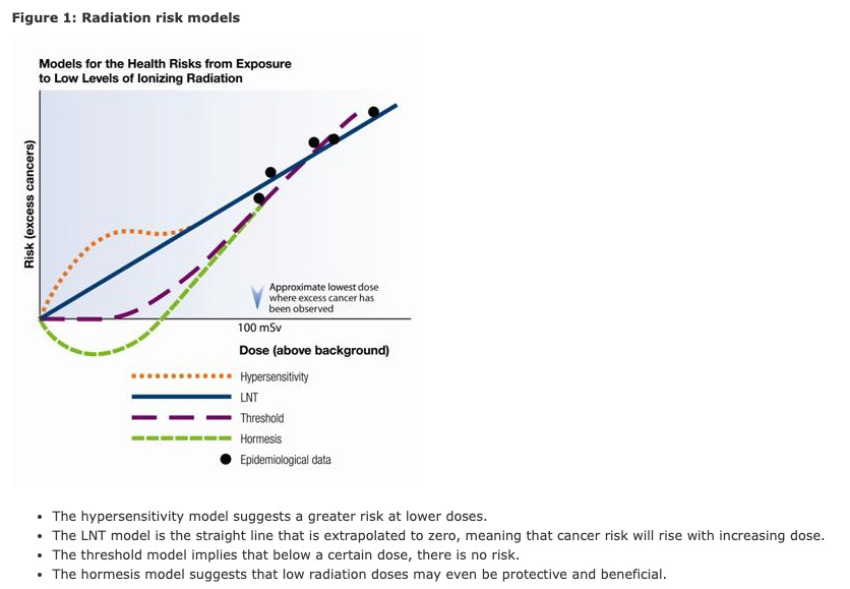
Radiation and Health Risks
CT scans represent one of the most significant sources of diagnostic radiation. An individual low-dose chest CT scan meant for screening delivers 1.0-1.5 millisieverts (mSv) compared with 6.1 mSv for a diagnostic study and 0.1 mSv for a chest X-ray. To put that in context, an average American receives approximately 2.4 mSv/year, with wide variation from natural background exposure based on local altitude, terrestrial radiation, and radon.
An environmental study of the entire US population displays a substantially longer life span among individuals with higher background radiation exposure. This observation has spawned the hormesis theory, which suggests a beneficial effect of low-dose radiation exposure.
How do we estimate risk? Let us begin with the most “accepted” model, the linear no-threshold (LNT) hypothesis of radiation carcinogenesis explained to a 1946 Nobel Prize audience by Hermann J. Muller. He predicted that even the tiniest doses of radiation would cause irreversible genetic damage. Muller’s evidence was based upon experiments examining transgenerational phenotypic observations in Drosophila (fruit flies), performed long before DNA was understood to be the source of transmission of genetic information. Later publications allege that Muller deliberately misinformed his Nobel prize audience regarding critical errors in his research data.
The LNT model hypothesizes a straight-line extrapolation from the highest doses of radiation associated with excess cases of cancer down to a small dose at baseline.
High dose radiation produces double-strand damage to chromosomes. One diagnostic measurement after radiation exposure involves cytogenetics to count the number of circular “minute” chromosomes seen after exposure. Gross chromosome breaks are thought to be irreparable. The same is not true of base-pair damage caused by lower radiation or toxin exposure. DNA repair is remarkably efficient, e.g., repairing DNA damage caused by cisplatin (a chemotherapy drug) within 48 hours after infusion. Repair of DNA lesions would theoretically shift the linear exposure/risk graph downward at low-dose exposures.
Another important consideration regarding radiation-induced cancers is patient age. Typically, there is a long latency period between radiation and cancer onset. Accordingly, the older the patient, the lower the anticipated duration of anticipated survival and the risk of subsequent cancer.
Many physicists in the US today repudiate the LNT theory. While there is strong data demonstrating powerful carcinogenesis with high-dose radiation (atomic bomb explosion, nuclear reactor accidents, radiation therapy, etc.), epidemiologic evidence is absent for a measurable carcinogenic effect at the low radiation doses (below 100 milli-Sieverts) that typically used in CT diagnostic imaging and screening.
 You can find a more extensive explanation of this graphic here.
You can find a more extensive explanation of this graphic here.
Consensus statements assert that the LTM theory is not “established science” for low radiation doses.
“below 50-100 mSv (which includes occupational and environmental exposures) risks of health effects are either too small to be measured or are non-existent.”
Health Physics Society position statement 20101
“The risk of harm from effective doses of less than 100 mSv is a highly controversial topic. At the effective doses associated with CT (approximately 1–12 mSv), the risks are extremely small or may in fact be zero.”
Summit on Management of Radiation Dose in Computed Tomography (CT) 2011
‘’ At the present time, epidemiological evidence supporting increased cancer incidence or mortality from radiation doses below 100 mSv is inconclusive. As diagnostic imaging doses are typically much lower than 100 mSv, when such exposures are medically appropriate, the anticipated benefits to the patient are highly likely to outweigh any small potential risks.“
Dr. Bindman and Alara
Dr. Smith-Bindman parlayed her study into a productive academic career, garnering long-term National Cancer Institute grants for her “CT Collaboratory” research project, designed to investigate CT imaging practices, to set, regulate and implement quality standards to minimize CT radiation exposure. Some might argue that her work reached its apogee on Christmas Eve, 2020 when the Centers for Medicare and Medicaid Services (CMS) awarded a sole vendor cooperative agreement to a startup company supporting the
“planning, technical assistance, and reporting needs related to submission of a fully developed and tested radiology measures to the 2021 Measures Under Consideration (MUC) List in May 2021.”
The company was Alara Imaging Inc; its two primary founders, Dr. Bindman and her husband. When I found out who the Alara executives were, I became concerned.
Conflicted Interests
Alara was incorporated in May 2020, months before the CMS sole-vendor cooperative agreement, to
“Optimize patient care through data analytics … lowers patient radiation doses by up to 40% without compromising image quality. …aligns payors and providers to reward exceptional care …[and] help physicians earn up to 18% more in CMS reimbursement.”
But the path to a company became much earlier, in 2014, following testimony from Smith-Bindman. Congress passed HR 4302 which
“delays the large cuts in Medicare called for by the Sustainable Growth Rate (SGR) if imaging facilities meet new requirements for stricter patient radiation dose safety controls in efforts to lower dose.”
HR 4302 provisions have never been implemented. CMS currently has no quality measures for either radiation dose or image quality. How, then, can Alara advertise that they will enhance reimbursement for imaging by 18%? The answer is regulatory capture – when the regulatory policy is driven by special interests in the market being regulated. More simply, it is “letting the fox guard the hens.”
Alara would provide CMS with data to support new, required quality measures. Since Alara would have written the quality measures and has proprietary software to assist providers in submitting data to CMS, it would be in the proverbial catbird seat, with a business advantage over potential competitors.
Under usual circumstances, other companies might have had an opportunity to provide competitive bids in response to a request for submissions. In this case, there was no such opportunity. Since the award was announced on Christmas Eve and went into effect on January 5, 2021, the possibility of objection was limited.
Why was Alara given a “sole-source vendor” cooperative agreement? A well-established principle is that government contracts should be awarded in a rigorous and open competitive bidding process. But...
“When government agencies solicit for bids using the sole source model, what they are implying is that the items or services they are looking to acquire can only be provided by one person or one company.”
While CMS awarded the contract to Smith-Bindman’s new company because “it is uniquely qualified to complete the work requested,” the assertion that Alara Imaging Inc. is “uniquely qualified” is questionable. Consider Smith-Bindman’s testimony before Congress in 2012.
“Additionally, a large number of dose-monitoring software companies have been created over the last several years. In California, a large number of these companies are marketing their products because they anticipate impending legislation that will require radiation dose information for each examination in the medical record.” [emphasis added]
One such company is Bayer Health, which provided the radiation dose data, using their “Radimetrics” software, for Bindman’s NCI research.
Entrepreneurs should profit from providing a beneficial public health service? But what if this benefit was a false alarm?
I believe that solid evidence suggests that it is highly unlikely that Alara's services will prevent 29,000 cancers. At best, there is weak scientific evidence that Alara’s services will prevent any cancers.
The 29,000-cancer estimate relies on the previously mentioned linear no-threshold (LNT) hypothesis of radiation carcinogenesis. Given the consensus by three professional organizations on the safety of radiation amounts for diagnostic studies, we must consider that the “modeled risk” is more hype than substance. In a tradeoff of harm and benefit, could the LNT hypothesis lead to harm? We need to look no further than the use of CT screening for lung cancer.
CT screening for lung cancer
Lung cancer (LC) is the most common cause of cancer death in both men and women in the US. If LC is identified at a small size and early stage by screening, as many as 80% can be cured by surgery alone. Unfortunately, LC typically is in an advanced stage at the first symptom. As asymptomatic LCs grow and metastasize to lymph nodes and other body organs, the chance of cure diminishes rapidly and can only be achieved with drug treatments with substantial toxicity and cost. The only approved method of early detection is a low-dose, non-contrast spiral CT scan.
The unsubstantiated belief that low-dose CT scans pose a significant risk of causing cancer has been widely cited to justify a rationale for delaying and restricting population CT-LC screening for those at high risk. For that, we can “thank” Robert J. McCunney, MD, an instructor in Pulmonary Medicine at Brigham and Women's Hospital and Harvard’s Harvard T.H. Chan School of Public Health
Dr. McCunney published three articles [1] in the journal CHEST, making dubious assertions about the radiation risk of CT screening for lung cancer. Philip Morris exploited his research to help avoid a legal obligation to pay for CT screening of their customers, who were put at higher risk of lung cancer by the sale of addictive and carcinogenic cigarettes. As he wrote,
“The findings indicate that a 55-year-old lung screening participant may experience a cumulative radiation exposure of up to 280 mSv over a 20-year period and 420 mSv over 30 years. These exposures exceed those of nuclear workers and atomic bomb survivors.”
Modern low-dose CT scans for lung cancer screening expose patients to approximately 1 mSv of radiation.
Dr. McCunney failed to report his activity as an expert witness to the editors and readers of CHEST - an obvious conflict of interest. When his false conflict of interest statement was reported, CHEST editors responded
“The author has reported to CHEST that there was an oversight in not addressing potential conflict of interest … he served as a consultant for attorneys in litigation and testified a year after the publications were released. (Donovan v. Philip Morris (PM) Civil Action No. 06-12234-DJC).’
Oversight? While it is true that Dr. McCunney testified a year after his publications, he was retained as a paid expert witness long before their publication.
The favorable verdict obtained in this case freed the tobacco industry from the potential obligation to pay for CT screening approximately 40,000 of their customers in Massachusetts. An opportunity to prevent more than a thousand lung cancer deaths was lost.
In the final analysis, no reasonable person questions the ethical obligation for clinicians and radiologists to exercise prudence and diligence in medical imaging, particularly in the care of young people. I urge CMS, in its current evaluation of data provided by Alara, to show wisdom and restraint in not imposing injudicious regulations that discourage or deter cancer screening with the potential to save many lives.
[1] Radiation risks in lung cancer screening programs: a comparison with nuclear industry workers and atomic bomb survivors Chest DOI: 10.1016/j.chest.2017.03.027.
POINT: should radiation dose from CT scans be a factor in patient care? Yes Chest DOI: 10.1378/chest.14-3020
Rebuttal From Dr. McCunney Chest DOI: 10.1378/chest.14-3021


