
Disclaimer: My thoughts are based on a summary of a poster that describes the study in question. While the poster is said to be peer-reviewed it is unavailable online at this time. We reached out to the authors for the original information and have not heard back after five days. No abstract is currently available.
From a recent press release:
"Aromatherapy reduces post-surgical opioid use by half in hip replacement patients anxious before their operation, according to a new preliminary study being presented at the annual meeting of the European Society of Anaesthesiology and Intensive Care (ESAIC) in Milan, Italy (4-6 June)."
I wouldn't normally bother commenting on this particular study because it's just more of the same – unneeded ways to reduce the use of pain meds and after surgery – if it weren't so poorly conducted. And biased:
Opioids have sedative and analgesic effects and are widely prescribed to after surgery to control pain. They are also addictive. Drug overdose deaths involving opioids (prescription and non-prescription, such as heroin) have increased more than six-fold since 1999 in the US and nearly 600,000 people in the US and Canada have died from opioid overdoses over the past two decades.
Seriously? This is the same old BS where a link between short-term use of a drug like morphine is somehow responsible for the surge in overdose deaths. It's a bunch of nonsense. This is simply a trick, which is widely used by anti-opioid zealots to convince the public that legal pain medications are still driving the surge in drug overdoses, therefore further pushing their agenda that pain med prescriptions need to be driven down even further (1).
Talk about disingenuous. Illicit fentanyl is by far the main culprit (and of course, the authors know this), so when anyone combines "prescription and non-prescription" drugs it's nothing but a dishonest trick. One could similarly state that "deaths from Lipitor and non-prescription drugs" have skyrocketed and be both accurate and misleading at the same time.
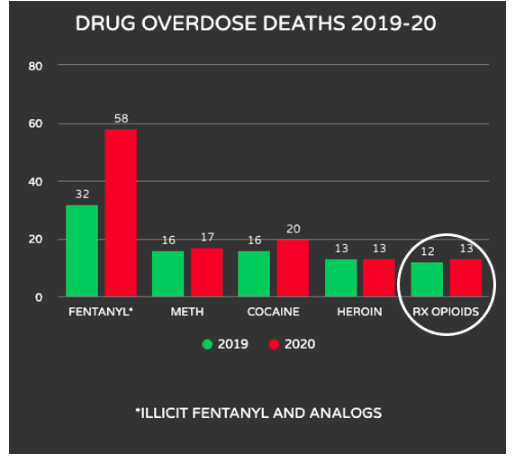
Overdose deaths of five classes of drugs of abuse: 2019-20. Deaths are expressed in thousands. Data: DrugAbuse.gov, CDC: Vital Systems Rapid Release: Overdose Death Counts
Let's take a look at some of the problems here. The researchers maintain that anxiety contributes to post-operative pain, which certainly makes sense; there is some evidence that aromatherapy can help with anxiety. They cite one paper during which 62 women undergoing Intrauterine insemination (IUI, a type of artificial insemination) were given lavender aromatherapy and their level of anxiety then measured. It should be noted that in the data table there are seven data points given, only two of which are statistically significant.
Those scoring as having a moderate level of anxiety or above are enrolled in the study, which is ongoing and aims to enrol [sic] 60 patients.
Aside from the small number of patients – only 25 were evaluated – this seems to be an example of selection bias. By picking the most anxious patients it is a given that their anxiety levels will fall more than that of those who are less anxious. Whether aromatherapy really helped the women undergoing IUI is impossible to tell.
Back to the current study.
Preliminary data on the first 25 participants (average age 60.6 years, 13 males and 12 females) is presented here. The primary outcome is the effect of aromatherapy on anxiety 48 hours after surgery. The baseline (pre-operative) anxiety score was similar in both groups (23.5 in aromatherapy group vs. 22.9 in placebo group).
The reduction in anxiety may or may not be significant; there is no way to tell.
"Total opioid use in the first 48 hours after surgery was 50% lower in the aromatherapy group (12 OME) than in the placebo group."
A couple of questions here.
In the absence of data it is impossible to tell whether this number is statistically significant. But more importantly:
Who determined the morphine doses that were given post-operatively? Was it the doctors doing the study or were the patients requesting it? If it's the former the study is automatically meaningless. If doctors are conducting a study to demonstrate that morphine can be reduced don't you think that is a pretty good incentive to give less of it?
What’s wrong with some Versed or Valium instead?
Nothing [my emphasis]:
Benzodiazepines can sometimes be very useful adjuncts for managing pain in patients who are already taking opioids, and when properly managed, there is no reason why benzodiazepines and opioids cannot be safely used together. Because benzodiazepines can potentiate the narcotic and respiratory depressive effects of opioids, proper management requires practitioners to be very careful with the dose and frequency of the benzodiazepine prescribed, educate their patients accordingly, and monitor them for side effects.
Jeffrey Singer, a practicing surgeon and ACSH advisor
If I'm in the hospital recovering from hip surgery I don't want flowers. I want monumental amounts of morphine and Valium coursing through my veins so that I am blissfully unaware of any pain I might otherwise suffer as well as the 300-pound Greyhound Bus driver having explosive diarrhea in the bed next to me. He may or may not have chosen the right aroma but is certainly emitting the wrong odor.
Aromatherapy use is both safe and dangerous
1. Safe
No one can possibly argue that if the scent of lavender calms post-op patients then they should have the option to use it. Whether the effect is real, a placebo or just a pleasant distraction doesn't matter. It's a fine option for people who want to try it.
2. Dangerous
Anyone following the issue of pain (mis)management knows full well that in today's hysterical anti-opioid climate anything – ridiculousness is welcome – that can be used in place of opioids will get good press and a pat on the back from like-minded colleagues (not too hard, please. It might hurt). I have written about (worthless) IV Tylenol, (dangerous and less effective) high-dose ibuprofen, (unproven and probably worthless) Neurontin, and (may God help you if you ever end up in the ER there) a hospital that uses a pranic healer and wandering harpist. (The hospital is St. Joseph’s Regional Medical Center in Patterson, NJ, which claims to be "on the leading edge" of the effort to control narcotic addiction." Should you be suffering from a painful affliction and find yourself in the vicinity I suggest that you might be wise to run in the opposite direction as quickly as possible. Then when you get there, keep going.)
While this may sound amusing keep in mind that both doctors and hospitals are under enormous pressure to avoid prescribing opioids, so we see the incursion of the faux treatments I mentioned above. Just like the CDC guideline on opioid prescribing quickly became laws and standard medical practice, it is all but guaranteed that we will see more nonsense, feel-good, evidence-deficient crap forced on patients, who do not want some half-baked alternative treatment. That is the real danger.
Our drug laws smell worse than the contents of the Greyhound driver's bowels.
NOTE:
(1) Please believe that the zealots want opioid prescribing to be even lower. In a recent debate about the causes of today's opioid problems, during which Dr. Jeffrey Singer absolutely obliterated PROP-bot Dr. Adrienne Fugh-Berman, Singer got her to admit that she thought that if all opioid prescribing ceased then drug overdoses would decrease, even though the prescription rate has dropped 60% since its peak in 2011 during which time overdose deaths have skyrocketed. For a moment I thought I must have walked into the comedy club next door. I will be writing about the debate, such as it was, soon.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.



{kind=link}