
“Protection of children’s health requires that health professionals understand the multiple harms to children from climate change and air pollution and use available strategies to reduce these harms.”
I will take these concerns in turn.
Climate Change
Let’s be clear; climate change has the potential to wreak havoc on the planet. Each of us (and certainly not just health professionals) is responsible for doing what we can to slow its progress. It’s got to be us, not just them.
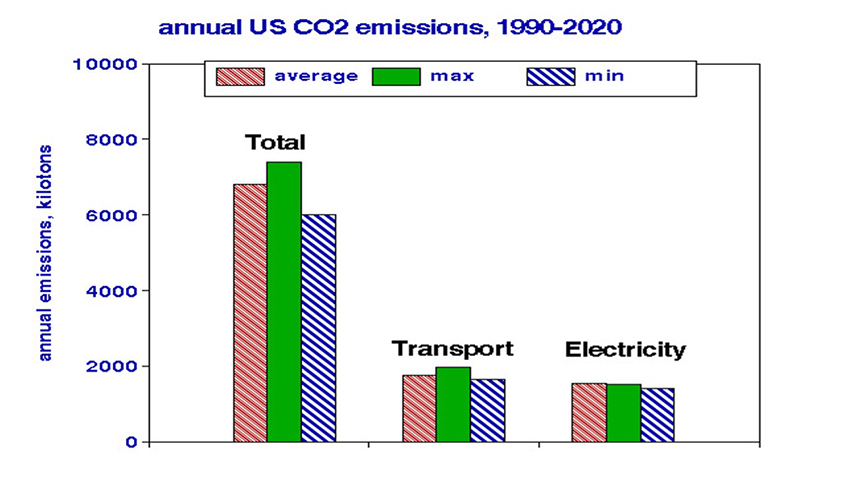 Now, let’s get real with some numbers. The available data on CO2 emissions show that transportation and electric power sources contribute only about half of the US total. Switching from gas to electric-powered vehicles shifts emissions within those sectors. Cutting powerplant emissions in half, which is wildly optimistic, only reduce total emissions by 11%.
Now, let’s get real with some numbers. The available data on CO2 emissions show that transportation and electric power sources contribute only about half of the US total. Switching from gas to electric-powered vehicles shifts emissions within those sectors. Cutting powerplant emissions in half, which is wildly optimistic, only reduce total emissions by 11%.
To meet international climate goals would require emission reductions throughout the economy, including our personal contributions. As individuals, we might:
- Cut back on space heating and air conditioning.
- Install solar panels and reflective roofing materials.
- Walk more and drive less.
- Cut back on manufactured purchases.
- Plant trees.
CO2 is not the only greenhouse agent. Methane (CH4 or natural gas) is many times more effective at trapping heat, and reducing its emissions is cost-effective rather than an expense since pipeline leakage is a significant source. A nationwide ambient CH4 monitoring program would identify sources and track progress in reductions – but would probably require EPA to identify methane as an air pollutant of concern.
An air pollution primer
Air pollution is a byproduct of an economy that satisfies our needs and demands; the marketplaces of institutions and individuals both have a say.
The traditional emphasis has been on combustion sources, reflecting
- The composition of fuel - sulfur, nitrogen, metallic trace elements such as lead
- The efficiency of combustion - unburned carbon [EC], carbon monoxide [CO], oxides of nitrogen [NOx]
- Downstream compounds formed in the atmosphere - ozone [O3], organic carbon [OC]
Each category releases pollutant gases and particles with differing potential health effects.[5] Although CO affects our oxygenation ability, gaseous pollutants primarily act as respiratory irritants with minimal long-term impacts. The effects of inhaled particles depend on where they deposit within the respiratory system, controlled by particle size, and what they do when they get there, as controlled by chemistry.
EPA has chosen to focus on PM2.5, defined as particles whose mean diameters are less than 2.5 μm regardless of chemical composition, and the rest of the world has followed suit. Combustion sources contribute to PM2.5 in different ways, but it doesn’t matter from a regulatory perspective with one important stipulation: only outdoor air quality is regulated. We spend > 90% of our time indoors, and surveys have shown that, on average, children now play outdoors only a few minutes per day.
About 50% of outdoor air pollutants penetrate indoors, mingling with household dust, cooking odors, candle smoke, second-hand tobacco smoke, air fresheners, and pet dander. Consider that about 70% of US households have a pet, but only about 13% of the population smokes regularly. Indoor air pollution can be more important than outdoors but has never been considered in the epidemiology studies that support air pollution regulation.
You might ask why we do not have enough data on indoor air quality and PM2.5 constituents to perform adequate epidemiological studies? Answer: because those pollutants are not regulated. And why are they not regulated? Answer: because regulatory agencies that control the funding for monitors lack data on their health effects. This syllogism has been with us since the 1970 Clean Air Act.
Several epidemiology studies are relevant.
- For a month, personal samples of PM2.5 constituents were collected daily from 40 urban fifth-grade asthmatic children. Their symptoms were associated with EC but not with local PM2.5 or sulfur.
- My studies of longevity in a cohort of about 70,000 US veterans found strong associations with vehicular traffic and EC but not with ambient PM2.5.
- Second-hand smoke exposure in residents was investigated in 28 families in New York City in terms of real-time effects on PM2.5. Average indoor concentrations were 24 μg/m3 and 15 μg/m3 for exposed and unexposed children, respectively, much higher than outdoor community levels.
These findings indicate the folly of focusing on (outdoor) PM2.5 as the major indicator of air pollution health effects. Nevertheless, it is helpful to consider trends in PM2.5 emissions by source categories, as well as time-dependent linear regression analysis.
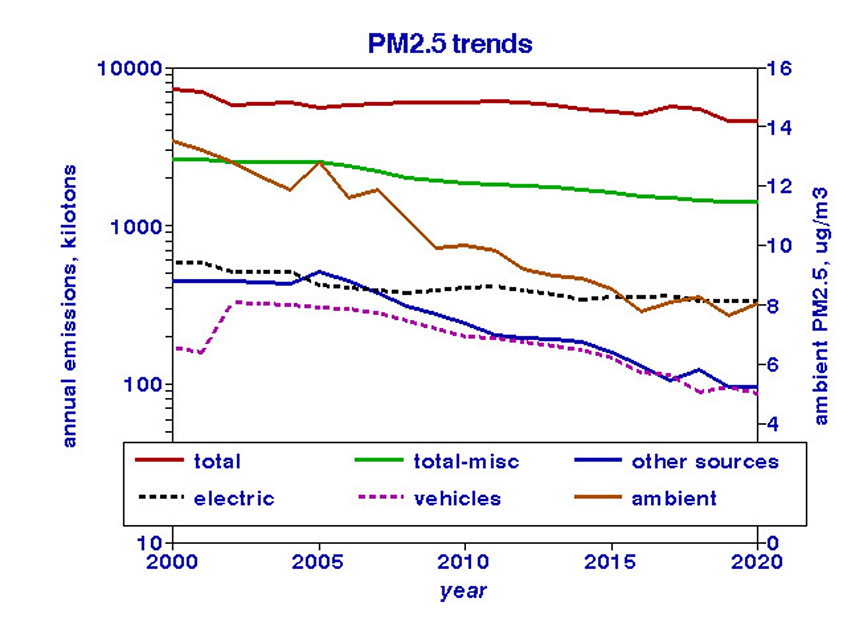 Trends in annual emissions of PM2.5 by source type compared with average ambient monitored levels, as reported by the US EPA.
Trends in annual emissions of PM2.5 by source type compared with average ambient monitored levels, as reported by the US EPA.
Ambient trends follow those for vehicles and other emission sources but not electric power sources, contributing roughly half as much to ambient PM2.5 as other sources. My analysis found that reducing vehicle and other emission sources to zero would still leave an ambient PM2.5 of 4.8 μg/m3, presumably from “natural” sources not amenable to regulation.
Exposures to community air pollution are largely beyond individual control, but there are things we can do:
- Buy low-emission vehicles and use battery- or human-powered outdoor appliances such as lawn mowers, leaf blowers, and hedge trimmers.
- Urge local government and school boards to do likewise. 99% of US school buses are fuel-powered and can expose children to exhaust fumes.
- Pressure state authorities to monitor and limit tailpipe emissions from diesel-powered vehicles.
- Eschew NIMBY to permit small-scale green facilities like wind turbines and solar panel arrays in your neighborhood.
Enter COVID-19
Many cities were locked down early in the pandemic, curtailing traffic and commercial activities and improving local air quality. Although it seemed logical to investigate any concurrent health effects, by and large, no one was outdoors to reap the benefits. Instead, indoor activities became more intense, and actual air pollution exposures were even more problematic. The CDC discusses increased ventilation to reduce indoor virus concentrations without mentioning the role of outdoor air quality.
So, where does all of this leave us?
- The current focus on reducing power plant CO2 has no chance of slowing down climate change. We need an “Operation Warp Speed” to deal with the increasing warmth we are experiencing and its ensuing effects.
- Carbon dioxide is not the only greenhouse agent of concern; methane has been neglected.
- Black carbon particles pose a double whammy: greenhouse effects and human health risks from inhalation.
- Expecting that reducing outdoor PM2.5 without considering indoor air pollution would improve long-term human health is a fool’s errand.
- Staying indoors to reduce COVID exposure requires more attention to indoor air quality.
- Increasing ventilation rates requires attention to outdoor air quality.
We have met the enemy, and he is us. Walt Kelly


