
Ask any chronic pain patient about gabapentin (Neurontin) as a replacement for opioids and you'll probably get one of two reactions: Laughter or tears. Yet, the drug, originally intended to treat seizures, and subsequently found to be useful for controlling nerve pain and restless leg syndrome has been pushed (along with miscellaneous other useless drugs and techniques) as a safe and effective alternative to legitimate opioid analgesics drugs. It is neither. A new JAMA article makes this painfully obvious.
Using a useless drug?
Bridget M. Kuehn, MSJ, writing in JAMA Medical News & Perspectives primarily focuses on how gabapentin is increasingly contributing to the soaring (1) drug overdose death toll but does not ignore the fact that off-label use of the drug to treat non-neuropathic pain is lacking in evidence, perhaps on an unprecedented scale.
In her article, Ms. Kuehn quotes a number of experts. Don't be surprised if you are surprised. [My emphasis]
“Gabapentin, by some estimates, is more widely prescribed off-label than what it is indicated for...We really don’t have data on what efficacy and dosages look like for this off-label use.”
Matthew Ellis, Ph.D., MPE, Washington University School of Medicine
If this isn't a red flag I don't know what is.
“Physicians have been afraid to prescribe opioids for fear that they will be contributing toward opioid misuse and abuse or that the Drug Enforcement Administration will prosecute them for prescribing opioids...There’s been a significant movement to nonopioids and gabapentin because it is believed by most physicians that it is not abused and that it is less harmful.”
Lynn Webster, MD, Center for US Policy
Isn't that wonderful? Physicians living under a cloud of fear and terror. From their own government. Let's give CDC, DOJ, DEA, and PROP our heartfelt thanks for destroying liberties and lives. Nice job, idiots.
“People are trying to use things other than opioids, and there aren’t a lot of options when it comes to medication for pain”
And
“The elephant in the room is the role of the pharmaceutical industry in the growth of gabapentinoid prescribing...We are living in the world created by that push for off-label use.”
Christopher Goodman, MD, University of South Carolina School of Medicine Columbia (2)
Additionally, Dr. Goodman co-authored an article, "A Clinical Overview of Off-label Use of Gabapentinoid Drugs" in a 2019 JAMA Special Communication in which the authors concluded:
The evidence to support off-label gabapentinoid (3) use for most painful clinical conditions is limited. For some conditions, no well performed controlled trials exist. For others, one or several placebo controlled studies have been published, but results have generally shown the drugs to be either ineffective or only modestly and inconsistently effective.
And I wrote a mini-review on the utility (lack thereof, really) of Neurontin in managing pain in 2019. (See Neurontin: The Darling Of The Anti-Opioid Crowd. But Does It Work?)
So, it is safe to say that, aside from certain neuropathic conditions gabapentin fails miserably when used off-label for pain, something any pain patient who has been denied opioid therapy will tell you.
Someone who did just this is Crystal Lindell, a pain patient who wrote of her experiences with the drug (and the doctors who shoved it at her, in a 2021 column on the Pain News Network site:
When gabapentin didn’t help with the pain, I went back to my doctor and told him as much. He increased the dose, while assuring me that that was all that was needed.
Wash, rinse, repeat, until I was on the highest allowable dose. Still with no relief.
Crystal Lindell, PNN 12/10/21
That's some mighty bad medicine, according to Chuck Dinnerstein, our Director of Medicine:
Gabapentin does not follow the more is stronger or better rule of thumb that physicians apply to other drugs. As a result, the dosage of gabapentin is increased and continually oversaturates receptors rather than producing a stronger response.
C. Dinerstein, M.D., Private communication 9/12/22
To digress for a moment, Isn't it funny that PROP fails to acknowledge the lack of viable options during any of its anti-opioid screeds? The group (falsely) maintains that opioids don't work for chronic pain, yet offer no useful alternative. Is the following the best they can do?
[Tylenol] is a very weak painkiller. I completely agree with you that it's, it's very weak painkiller. It actually has, um, can be extremely effective when it's combined with a nonsteroidal anti-inflammatory drug. It can actually increase the effect of the NSAIDs. So it's kind of a magic combination combining Ibuprofen or another NSAID, um, with Tylenol, even though the Tylenol on its own is really quite weak.
PROP member Adriane Fugh-Berman, Transcript from a Debate with Jeffrey Singer, June 7th, 2022
Fugh-Berman's cutting-edge medical advice involves combining a 67-year-old virtually useless drug (Tylenol) with a 53-year-old drug (Advil) that many people can't even take. How innovative!
Improper use and abuse: Unintended (but not unforeseen) consequences
if you predicted in 1993, when gabapentin was approved, that it would be used three decades later as a primary pain medication you could have possibly become the founding member of QAnon. Yes, it's that crazy, But because of the CDC- and DEA-sponsored mad rush away from opioids many doctors adopted an "it probably won't help but at least it won't hurt" mindset if only to get pain patients out of the office with something. This is reinforced by prescribing data. Between 2004 and 2019 the number of prescriptions for gabapentin rose from 18 million to 45 million – an increase of 250% – much of which was certainly a result of opioid phobia. This has created its own set of problems: lack of efficacy and abuse.
It is more than a little ironic that in the thoroughly misguided attempt to get a handle on drug overdose deaths by imposing severe restrictions on opioid prescribing use (down by 60% and counting) gabapentin, the designated substitute, is being thrown at patients. And why not? After all, it is a Schedule V drug, along with other monsters like Lomotil and Robitussin AC. Gabapentin can be refilled up to five times, so it is not surprising that there is plenty of it around.
Which should be no surprise to anyone who was paying attention six years ago.
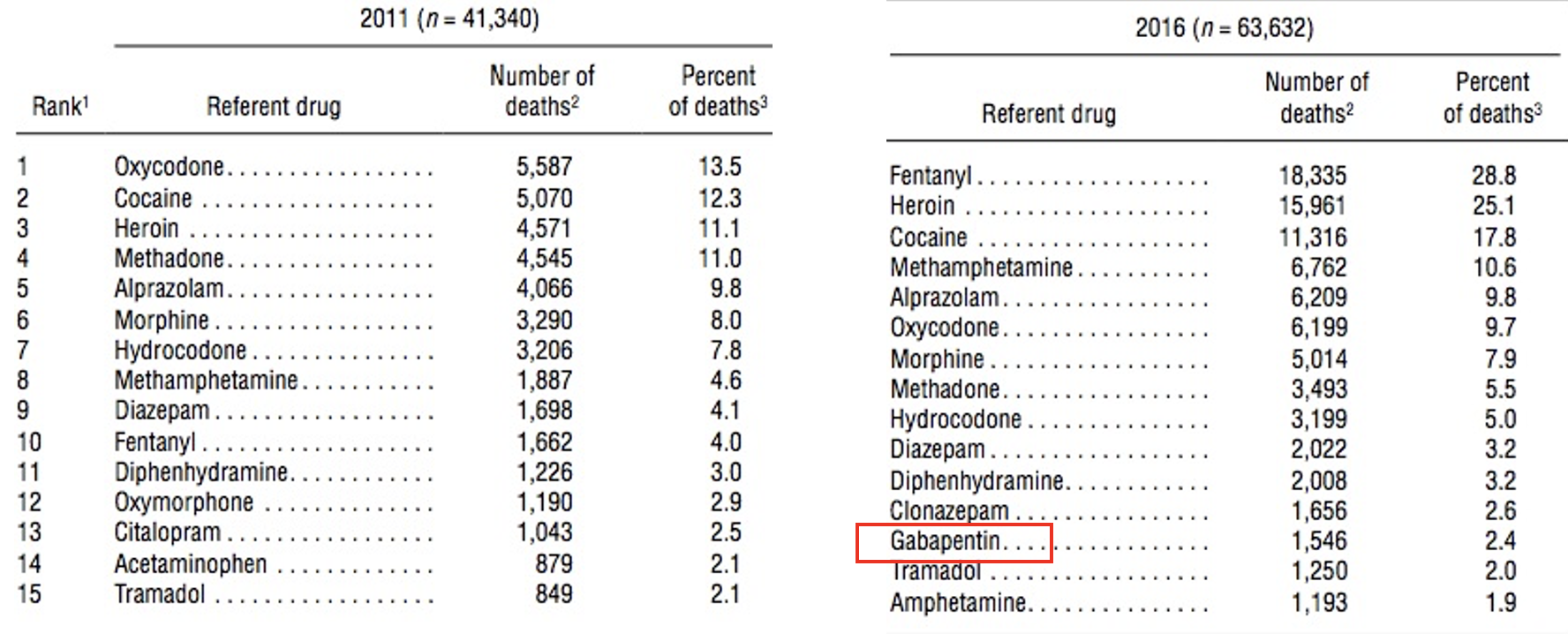
Neurontin (gabapentin) came out of nowhere and joined the list of the top 15 drugs involved in overdose deaths in 2016. How did a Parkinson's drug get there?? Source: National Vital Statistics Reports
Of course, once gabapentin abuse began it was virtually guaranteed to proliferate. It did. Even the CDC figured this out:
Although gabapentin is generally considered safe and is infrequently associated with overdose on its own, when used with other central nervous system depressants such as opioids, there is risk for respiratory depression, potentially resulting in death.
[D]ata indicate gabapentin exposures associated with intentional abuse, misuse, or unknown exposures reported to U.S. poison centers increased by 104% from 2013 to 2017...[A]mong 58,362 deaths with documented toxicology results, a total of 5,687 (9.7%) had gabapentin detected on postmortem toxicology. Gabapentin-involved deaths occurred in 2,975 of 5,687 decedents (52.3%) with a positive gabapentin test result.
Isn't it obvious that the more we continue to bungle the unwinnable "war on drugs" the result will be more and different abused drugs, more deaths, and more suffering for pain patients, who play no significant part in overdose deaths? (3)
My colleague Dr. Jeffrey Singer emphasizes what he calls "opioid prohibition," and how (as was the case with alcohol prohibition) when one drug is prohibited people will find something else that is less safe, in this case, fentanyl, heroin, cocaine, methamphetamine, and now gabapentin, which may be abused but also used for another reason:
I suspect gabapentin OD deaths are not from recreational use, but from pain patients who are in such agony that they take bigger and bigger doses to try to get relief. I suspect that doctors are increasing the dose when the initial dose is ineffective, that sends some patients the message to patients that it's safe and OK to increase the dose until you achieve the desired result.
Jeffrey Singer, M.D. Private Communication, 9/14/22
As has been the case since fentanyl hit the US in 2013 there are still lessons to be learned about what really happens when legal and necessary medications are demonized and prohibited. How many more "drugs of abuse" will be futilely added to the DEA's hit list? How many more pain patients will continue to face a choice between living in agony and trying to quell it with whatever pharmaceutical crumbs are tossed their way?
Such unspeakable cruelty.
NOTES:
(1) Of course, it is illicit fentanyl that continues to be responsible for the vast majority of OD deaths and will probably maintain first place until something worse comes along.
(2) Isn't it ironic that the pharmaceutical industry, which has been blamed for causing the opioid crisis, is now blamed for pushing hard for a replacement drug? Just asking.
(3) The term "gabapentenoid" is used because there are several structurally similar drugs that form a class.. People generally hate all of them.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


