It is undoubtedly clear from the graphic that the respiratory disease season has had an early start. It is equally clear that extrapolating from those two weeks is fraught with uncertainty, not only for the trajectory but for its height – the caseload.
Let’s begin with the biological why
We do not know, but infectious disease experts have offered some possible reasons. Here is the CDC data from last year concerning the strongest of the current drumbeats RSV.
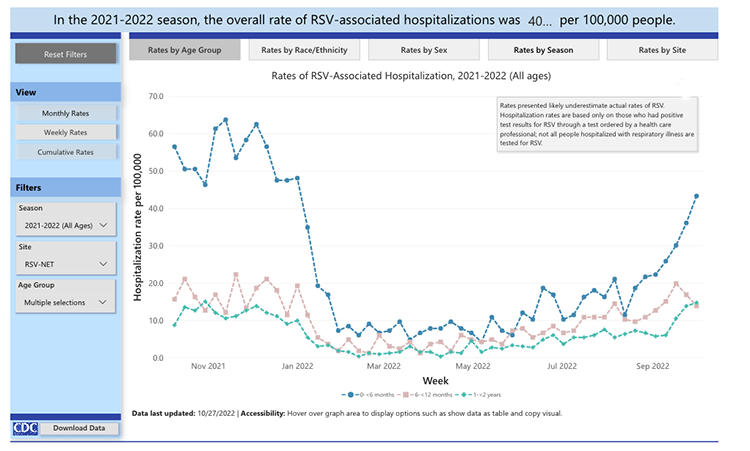
The numbers of cases are higher this year, by roughly 60 or 70%, but last year’s peak period seems to have been early fall through early winter, just as it seems to be playing out today. The trajectory of the disease, its ups, and downs, seem similar, but the number of cases appears to be rising. Experts in infectious disease feel that the measures we took to flatten the curve for COVID may have increased the reservoir of susceptible individuals, especially children to age 2, who were not exposed to RSV to the same degree as in previous years. Social isolation and masking may have had “downstream” effects – a biologically plausible but untestable narrative.
The Burden of RSV on patients and hospitals
According to the CDC, 2.1 million children under age 5 develop RSV. 58 to 80,000 require hospitalization, a hospitalization rate of 3.8%, and there are 100 to 300 deaths, a case fatality rate of 0.014%. Now, this fatality rate is, in fact, almost five times higher than fatalities from influenza for this age group. Still, it would seem that the public health threat of RSV is primarily on overwhelming hospital capacity.
For many years, long predating our concern over COVID, hospitals have been shedding pediatric beds. While the numbers vary geographically, since 2000, we have reduced pediatric beds by a third to a half. There are many reasons for this, including shifting care to outpatient services (as we see with adults), regionalization to specialized children’s hospitals, the lack of trained personnel, especially pediatric nurses, to “serve” those beds, and profitability. Most pediatric units require $1 million in subsidies to remain open, so our capacity to treat pediatric patients was capped.
Children are not “small adults.” Their physiology is in flux; their care requires specialized caregivers; again, not just pediatricians, but pediatric nurses and other specialists like pediatric infectious disease experts. Pediatric expertise is a challenging bottleneck to expanding care, shifting adult to pediatric beds without staffing those new pediatric beds with specialists doesn’t work. The hospitals’ ability to expand in response to much higher than normal admissions, as is the case for RSV, is limited – I would describe it as brittle.
While it is rarely mentioned, RSV can infect adults. In fact, roughly 60-120,000 adults over age 65 are hospitalized for RSV infections, and the global case fatality rate is 0.0025%. There has been little concern over possibly rising rates of adult RSV because that reservoir of hosts seems not to have been impacted by our COVID precautions. That makes sense because adults have been exposed to RSV for decades.
COVID
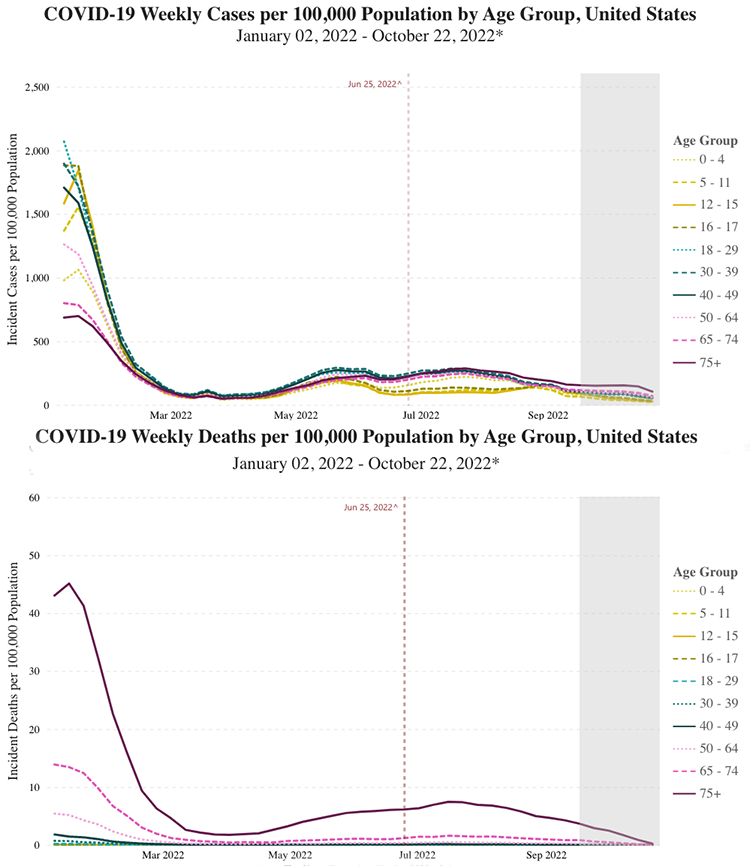
Here is the latest data from the CDC for COVID; as you can see, both cases and deaths have been down dramatically since the beginning of the year, and they continue to trend down during October.
Again where you live makes a difference in caseloads. Here in New York, COVID hospitalizations are up nearly 3-fold from October of 2021. But that number is dependent upon the denominator we choose. COVID hospitalizations are up roughly 30% compared to the nadir in September and 60% compared to the bottom in July.
ICU admissions, the capacity limitation for adult hospitalizations, have dropped dramatically, from 21% of admissions to 9%. Unlike RSV, there is a vaccine for COVID, and the latest versions have been formulated to treat the more predominant variants.
According to the Kaiser Family Foundation, overall COVID vaccination rates are steady at about 80% of the population, with about 23% of adults unvaccinated and not planning on getting vaccinated in the near or long term. About a third to a half of those already vaccinated are considering the booster. To what degree Americans choose to be “boosted” may well determine how that curve will change.
Influenza
Seasonal influenza is upon us, and as with COVID, a vaccination is available. Now the targets of the vaccine change every year, but we have the species that were active in the Southern Hemisphere as a guide to what may bother us now in the Northern Hemisphere. A New England Journal of Medicine study suggested that influenza vaccination tracked with COVID vaccinations and that once again, for any number of reasons, individuals declining COVID vaccination also rejected influenza vaccination. Roughly half of the population at risk vaccinate against influenza, more so among the elderly.
Here is the latest data from the CDC
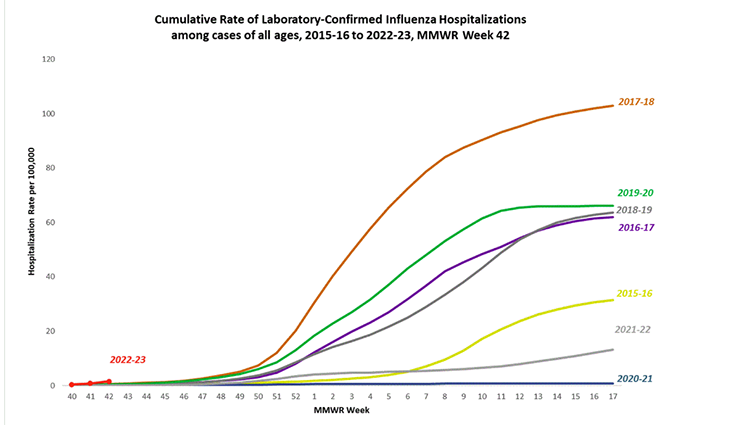
It is hard to extrapolate from those three data points, but you can easily picture this year’s influenza season following the same temporal trajectory of years past. As with COVID, a means to reduce hospitalization is within our reach, vaccination.
From my reading of the data, we will see that all three respiratory viruses result in hospitalizations. I think that the surge in RSV will be over as influenza and COVID cases rise, but in any event, the hospital capacity for treating pediatric RSV is already baked in and will not impact the ability of most hospitals to respond to a “surge” in COVID or influenza hospitalizations. The phrase “tripledemic” is click-bait, attention-grabbing, fear eliciting, casting more shade than light. Here is the real bottom line. The degree to which our fellow citizens roll up their sleeves to get vaccinated against the latest COVID and influenza variants will directly impact the stress on our hospitals and medical staff. The season of viral respiratory illness is upon us; a means to flatten the curve is at hand; we just have to do it.
Source: Why everybody you know is sick right now, VoxCare

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


