
The data comes from our Midwest, the Indiana Network for Patient Care, an extensive clinical data repository on Indiana's citizens. Vaccinated individuals were matched for “age, gender, race/ethnicity, zip code, and the number of coexisting conditions” with an individual with an established COVID infection. The cohorts of roughly 270,000 individuals in each group were well-matched with one another, although not wholly reflective of our national demographics. [1]
The outcomes of COVID infection or reinfection, all-cause ED visits, hospitalizations, and deaths were recorded beginning 30 days after vaccination or infection.
“Six months after the index date, the cumulative infection rate in the vaccinated was 6.7%
… more than twice the rate in those with previous infections at 2.9%.
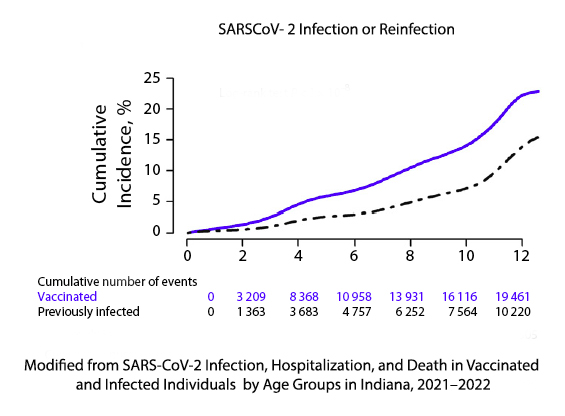 Naturally acquired immunity was more protective than vaccine-acquired immunity from infection. You can see the numbers of infected or reinfected in the case of naturally acquired immunity over 12 months. A ready explanation may simply be that naturally acquired immunity has more targets than the surgical precision of our mRNA vaccines. And a quick word of caution, the members of the naturally acquired immunity cohort had survived their COVID infection; everyone is not so lucky.
Naturally acquired immunity was more protective than vaccine-acquired immunity from infection. You can see the numbers of infected or reinfected in the case of naturally acquired immunity over 12 months. A ready explanation may simply be that naturally acquired immunity has more targets than the surgical precision of our mRNA vaccines. And a quick word of caution, the members of the naturally acquired immunity cohort had survived their COVID infection; everyone is not so lucky.
But before we rush out to schedule a COVID infection party or go to a crowded, indoor public event, there is some more data. All-cause emergency department visits were less among the vaccinated (6.7% vs. 5% for the vaccinated); same for all-cause hospitalization, 1.9% vs. 1.2%, and deaths, 0.51% vs. 0.32%. [2] And all of these values were statistically significant.
Are the findings clinically significant? That depends. First, naturally acquired immunity was more protective against (re)infection for all age groups. For all age groups, vaccination was more protective against the harmful impacts of those infections, ED visits, hospitalizations, and deaths. While increasing age, perhaps as the measure of fragility, is associated with increasingly poorer outcomes after COVID infection, the study failed to demonstrate a significant disparity in these outcomes between those vaccinated or naturally protected.
There were no death among children (defined as age 19 or less), which is important in the conversations surrounding the incidence of myocarditis from COVID or vaccination in this age cohort for males.
If you are willing to risk hospitalization, death, or prolonged illness (currently termed Long COVID), then naturally acquired immunity will be more robust in protecting you from a second episode. It will not be as protective from the outcomes of that second infection. This is a real-world example of the tradeoff between “an abundance of caution” and rolling the viral dice that may or may not be loaded by your underlying frailty as measured by risk factors or your access to care.
You may also wish to consider the consequences to those around you, your family, and neighbors. Infections at close quarters facilitate transmission to others. The children are disease influencers for COVID and a host of other respiratory illnesses they pick up from their peers – if you doubt this, ask a parent of a child starting daycare.
When it comes to COVID, I am a belt and suspenders guy. I had COVID in October, and I plan to travel in the next few months. I plan on getting my booster before I go. The bottom line for me is not an abundance of caution; it is because shortly after contracting COVID, I had a pulmonary embolus that could have killed me. I choose not to take that risk again, and I think the booster is my way forward. What is your best way forward? There is no one-fit-all answer, but making a choice based on a political/social calculus rather than a health-based evaluation is for fools.
[1] 58.2% female, 87.9% White, mean age 38.9
[2] For those that like risk ratios or bigger numbers in general, there was a 33% greater chance of emergency department visits, 58% greater chance of hospitalization, and 60% greater chance of death among those with naturally acquired immunity
Source: SARS-CoV-2 Infection, Hospitalization, and Death in Vaccinated and Infected Individuals by Age Groups in Indiana, 2021–2022 American Journal of Public Health DOI: 10.2105/AJPH.2022.307112

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


