
Today’s villain is erythritol, a naturally occurring “sugar-alcohol” (polyols) used as a sweetener. It is not as sweet as sucrose, so it is typically used in far higher amounts in the “food chain” than in our fruits and vegetables. It is “poorly metabolized and mostly excreted in the urine,” making it a non-nutritive, natural, zero-calorie sweetener.
Before getting to the clinical data, consider whether the presence of erythritol is a bioplausible mechanism for coronary artery disease. For this, the researchers considered enhanced clotting. In a laboratory, in vitro model, adding erythritol to platelet-rich plasma at physiologic levels enhances platelet aggregation in a dose-response manner. And while the levels of erythritol were physiologic, platelet-rich plasma is, by definition, not physiologic, so we must consider the findings as interesting but certainly not overly convincing.
In an in vivo study of our friends, clotting after injury was also enhanced in mice. But again, similar is not the same, and at least one study suggests
“In particular for therapeutic studies, long-term effects, chronic disease conditions as well as rapid activation of the [central regulating signaling cascade of platelets], it is clear that any helpful observation and insight from the mouse models has to be closely validated for human platelets as details and modulation are often somewhat different.”
To put a human face to those studies, the researchers had eight subjects drink an “erythritol-sweetened drink (30 g).” Their narrative features a confusion of units. They begin by expressing the baseline of 3.84 µM (micromoles) but then express the peak, 5.85, in mM (millimoles). But a 30gm dose of erythritol doesn’t [1] contain that high an amount even if all of it is in your circulation. This raises a new concern, are their calculations incorrect, or is there another endogenous source of erythritol? There is, in fact, another source, glucose, and as this study of weight gain reports,
“We also found the concentration of erythritol was higher in the group with higher glycemia compared with the group with lower glycemia at study baseline.”
Erythritol can enhance clotting, but does dietary ingestion enhance clotting in humans under normal physiologic conditions? We do not know, and the study does not convince.
The study’s clinical data begins by reporting an “untargeted” analysis of patients undergoing elective cardiac evaluation, meaning individuals symptomatic for cardiovascular disease. They identified erythritol among the many polyols associated with “major adverse cardiovascular events (MACE = death, myocardial infarction and stroke).” It had the most significant association of the polyols with MACE, raising the concern that it might play a role in this outcome disparity. Of course, a plausible alternative theory might simply be that it is the most widely used polyol in foods or that it arises naturally, so the association may just be a confounder.
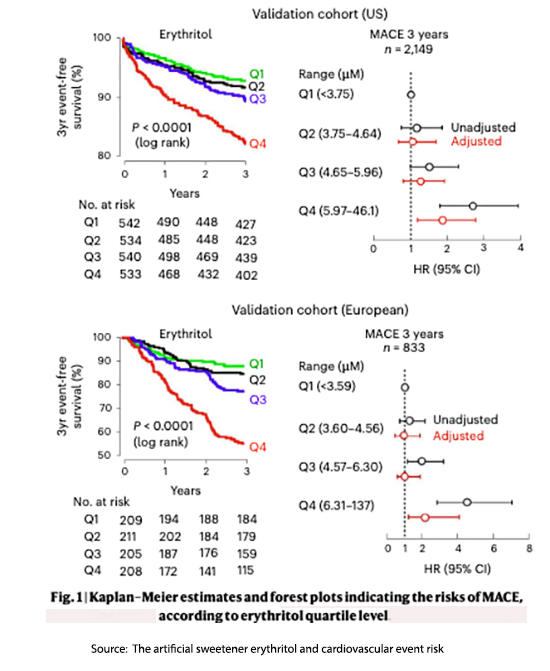 They validated their initial findings by looking at two additional cohorts of cardiovascular patients, one from the US and the other from the EU.
They validated their initial findings by looking at two additional cohorts of cardiovascular patients, one from the US and the other from the EU.
Here is the data demonstrating that diminishing survival as the plasma level of erythritol increases – only the group with the highest erythritol levels (Q4) had a statistically significant greater association with MACE.
Are there any other differences between the lowest (Q1) and highest (Q4) groups?
Indeed, but one has to look elsewhere in the online supplemental data. Among the differences, the US Q4 was significantly (statistically) older, with higher incidences of diabetes, coronary artery disease, myocardial infarctions, congestive heart failure, and greater triglycerides. Their LDL cholesterol was significantly less, as was their HDL. The EU Q4 was also statistically older, with a higher incidence of diabetes and heart failure. They smoked less than their Q1 colleagues and had lower LDLs. The groups differ in more ways than just plasma erythritol levels. Adjusting for these differences removes much of the disparity in outcomes.
In his takedown of the study, Dr. Peter Attia makes an additional very critical point.
“The investigators did not collect any data on erythritol intake from any of their human cohorts, so we have no way of correlating consumption with MACE risk because we have no way of knowing which participants were regularly consuming erythritol-containing foods. Indeed, Witkowski et al. note that the vast majority of their study participants were enrolled prior to erythritol becoming a common sweetener and food additive. … In other words, this study provides no evidence whatsoever that the association between circulating erythritol and MACE has anything to do with dietary erythritol intake.”
Well, that is undoubtedly problematic, especially given the much greater presence of individuals with diabetes in the Q4, higher-risk group.
Once again, we have a click-bait, fear-mongering headline that serves the needs of platforms earning money from views but does little to serve the public in their quest for healthy dietary choices. Here are the media ledes.
Study Links Sugar Substitute Erythritol to Blood Clots and Heart Attack
The findings are raising eyebrows about the sweetener. Prevention
Could our love affair with sugar and artificial sweeteners literally break our hearts LA Times
Popular artificial sweetener erythritol linked to higher risk for blood clots PBS
I will leave the last word to the researchers, although I will add the emphasis.
“In summary, the present studies suggest that trials investigating the impact of erythritol specifically, and artificial sweeteners in general, with appropriate duration of follow-up for clinically relevant outcomes, are needed. Following exposure to dietary erythritol, a prolonged period of potentially heightened thrombotic risk may occur.”
[1] Erythritol has a molecular weight of 122.2 gm/mole. A 30-gram dose will therefore contain .245 moles. When distributed across the 2.5 liters of plasma in our circulation, that comes to 98 µM/ml. In mM, that would be, 0.00098
Source: The artificial sweetener erythritol and cardiovascular event risk Nature Medicine DOI: 10.1038/s41591-023-02223-9

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


