
Erythritol is a naturally occurring sugar alcohol found in some fruits and fermented products. It is unique in that it has no caloric value but roughly 70% of sugar’s sweetness, making it a natural to be used in low-calorie foods. While no safe levels have been established because erythritol:
- It is naturally found in food
- It has been found to have no apparent effects on insulin or glucose
- Its safety has been demonstrated in studies of both animals and humans
Erythritol is “generally recognized as safe (GRAS)” by the FDA and the always more stringent EU. There is one further reason for that GRAS classification: humans produce erythritol, too. It is part of our metabolism of sugar, the pentose phosphate pathway. This pathway is more active in “response to oxidative stress,” glucose dysregulation, and in patients with known cardiovascular disease. That is part of why it is a molecule of interest.
The Study
The participants in the study were all patients undergoing cardiovascular evaluation; all patients had some current cardiovascular disease. The population was (obviously) enriched with cardiovascular disease, a two-edged sword. While this allows for identifying a small effect from erythritol, it also limits the ability to generalize the findings. Whatever was concluded about erythritol has no bearing on individuals without current cardiovascular disease.
In the study's first phase, 1,157 individuals undergoing cardiac catheterization had blood levels drawn and characterized for the presence of polyols (sugar alcohols) that include several sugar substitutes, such as erythritol, xylitol, and sorbitol. When followed for 3 years, individuals with MACE events had statistically higher levels of polyols – a sign of an association between polyols and MACE but not specific to erythritol.
In the study's second phase, the researchers analyzed the blood of two additional groups, again with cardiovascular disease, from the US and Europe. The blood analysis was more targeted, looking specifically at erythritol, and once again, those individuals with an increased risk of MACE had significantly higher concentrations of erythritol.
There are two difficulties with drawing any conclusions at this point. First, the blood samples used in the analysis were taken on entry to the studies and not repeated. There were no follow-up blood draws and no information on the participant’s diet. In fact, the researchers noted that the majority of participants were recruited before erythritol became a common food additive. We cannot tell whether the erythritol of concern was consumed; it may have been a product of the pentose phosphate pathway. In the words of Peter Attia, MD,
“In other words, this study provides no evidence whatsoever that the association between circulating erythritol and MACE has anything to do with dietary erythritol intake.”
The researchers stratified their results by those serum levels of erythritol. This leads to the second difficulty in drawing conclusions, the “apple to orange” comparison.
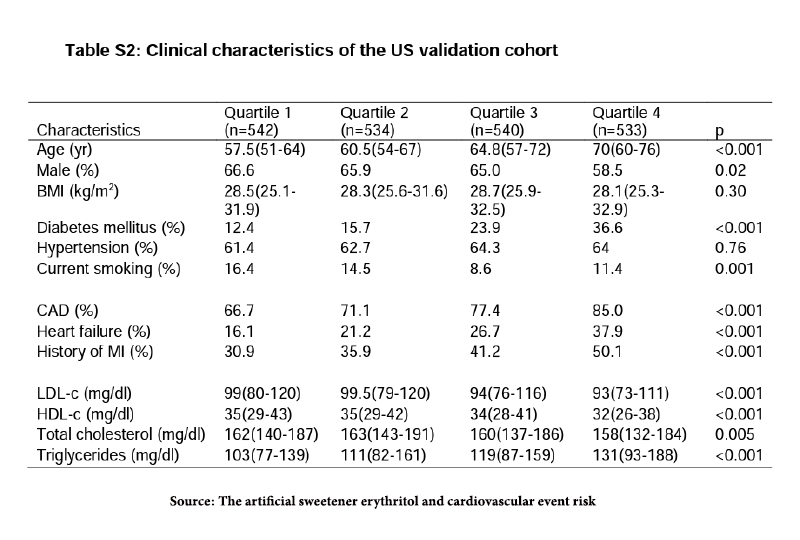
The results reported by the researchers compared Quartile 1 with the lowest erythritol levels, with Quartile 4 the highest. The differences between Quartiles 1 and 2 and 1 and 3 were insignificant, suggesting that there was no dose-response and that, if anything, there was a threshold erythritol level that, when exceeded, led to greater MACE. But take a moment to examine the differences between Quartile 1 and 4. The group with the highest erythritol levels also were older and had statistically more diabetes, hypertension, coronary artery disease, heart failure, and a history of MI. While the researchers might use statistical controls to lessen these disparities, they cannot actually control for the underlying physiologic changes. Quartile 4 had more risk than Quartile 1 irrespective of erythritol levels – levels also elevated in the presence of diabetes and age.
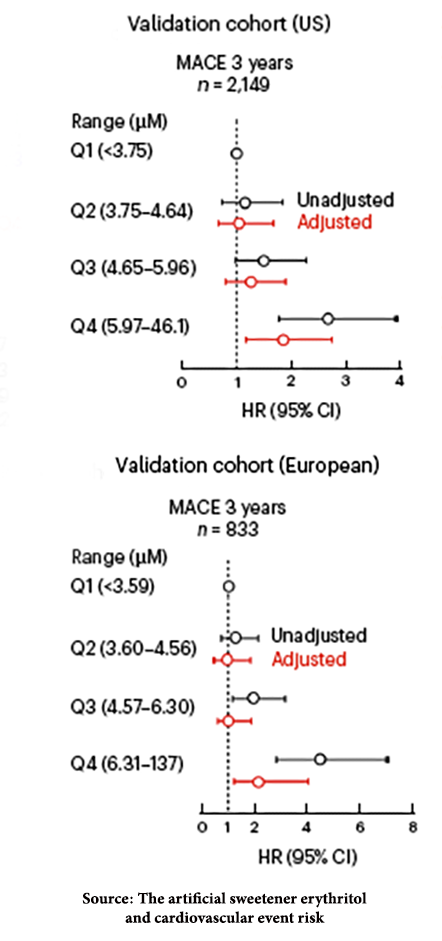
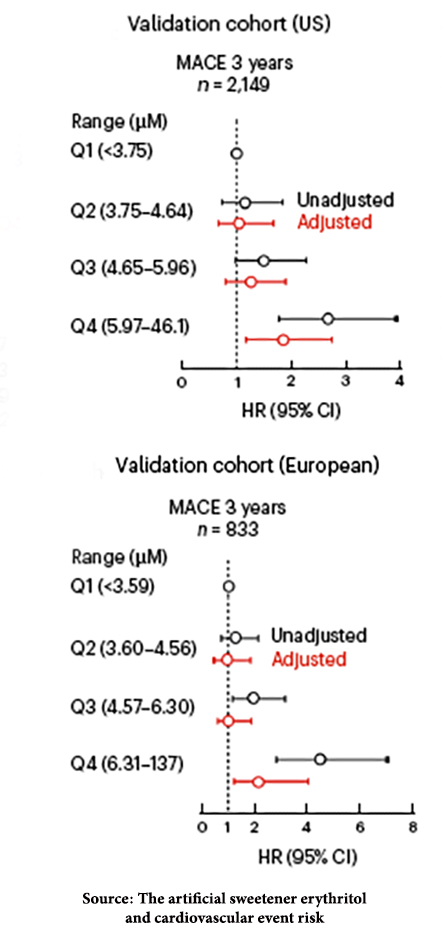 The researchers determined that higher levels of erythritol were associated with approximately a doubling of risk of MACE. The researchers were transparent in stating that this was an association, not a causal link. Not surprisingly, the popular press reported otherwise, a classic case of science being lost in translation.
The researchers determined that higher levels of erythritol were associated with approximately a doubling of risk of MACE. The researchers were transparent in stating that this was an association, not a causal link. Not surprisingly, the popular press reported otherwise, a classic case of science being lost in translation.
For those who wish to delve a bit deeper, age was a greater determinant of risk than erythritol in both the US and European cohorts.
Erythritol and blood clotting
The researchers suspected that erythritol might enhance clotting, a common pathway to MACE events. One study in which erythritol was added to platelet-rich plasma found that erythritol enhanced platelet aggregation. But like the population used to identify erythritol’s cardiovascular risk, the plasma used to find that enhanced clot-ability was enriched and not an actual physiologic concentration.
In another study involving mice, “erythritol sped the rate of clot formation relative to control solutions, though it is worth noting that serum erythritol concentrations in this experiment were over double the highest concentrations seen in the human discovery, US, or Europe cohorts.”
In the final phase of this study, researchers looked at how plasma levels of erythritol changed when “challenged” with dietary erythritol. Remember, none of the study participants had prior documented erythritol ingestion. Eight healthy individuals were asked to drink 10 ounces of 30 grams of erythritol after an overnight fast. Erythritol levels rose rapidly – more than 1,000-fold within 30 minutes – and remained elevated at 48 hours. But that was an enriched dosage. As other critics of the study point out,
“Erythritol-containing beverages and foods are typically consumed throughout the day, and not within a very short timeframe. …Moreover, erythritol is very often present within a food matrix that has a delaying effect on postprandial absorption. It is therefore questionable whether the reported plasma concentrations also occur under “real life” conditions.”
A typical drink in the EU can contain up to 4.8 grams of erythritol, so 30 grams in a 300ml dose works out to downing nearly a half-gallon to start your day.
A more critical takeaway
- The results demonstrate a correlation between circulating erythritol and MACE, but only at “especially high physiological” levels.
- Causality is unclear as it is with an observational study, including cohort studies.
- The study provides no evidence for the impact of dietary erythritol on MACE.
- “The authors were totally aware of this limitation and they also mention it in the discussion (“... these studies can only show association and not causation”) [and] …they emphasize several times that their results only apply to people with increased cardiovascular risk. In summary, the authors must be credited for not overstating the results of their study… Such a differentiated and transparent presentation is remarkable and (unfortunately) rather not the rule in nutritional studies.”
In a setting with significant uncertainty, the individual's decision to consume erythritol remains based on their understanding of the scientific data and risk tolerance.
Note: I would like to thank Dr. Hazen, the study's senior author, who graciously provided a non-paywalled copy of the study to base this article.
Sources: The artificial sweetener erythritol and cardiovascular event risk Nature Medicine DOI: 10.1038/s41591-023-02223-9
More hype than substance: erythritol and cardiovascular risk Peter Attia MD
Plasma erythritol and cardiovascular risk: is there evidence for an association with dietary intake? Frontiers in Nutrition DOI: 10.3389/fnut.2023.1195521

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


