
One of our standard medications used in caring for the critically ill is steroids, more specifically glucocorticoids. Early in the pandemic, a steroid called dexamethasone was used to care for hospitalized COVID patients and showed a benefit regarding the ultimate outcome, dying. A “standard” dose of dexamethasone was roughly 6-10 mg. The drug is safe and effective when used in “exacerbations of asthma and chronic obstructive pulmonary disease” – if a little is good, wouldn't more be better?
The RECOVERY trial is an ongoing individually randomized open-label trial of potential treatments for patients hospitalized with COVID. [1] Patients, age 18 or older, hospitalized for suspected or confirmed COVID with evidence of hypoxia (receiving supplemental oxygen with or without some mechanical support or having oxygen saturations <92% on room air) were enrolled. Patients with known contraindications of a short course of steroids were excluded. The primary outcome was the 28-day all-cause mortality.
“On May 11, 2022, the data monitoring committee recommended stopping recruitment to the higher dose corticosteroid comparison for patients who require no oxygen or simple oxygen only at randomization due to safety concerns.”
It was stopped two days later.
What Had They Found?
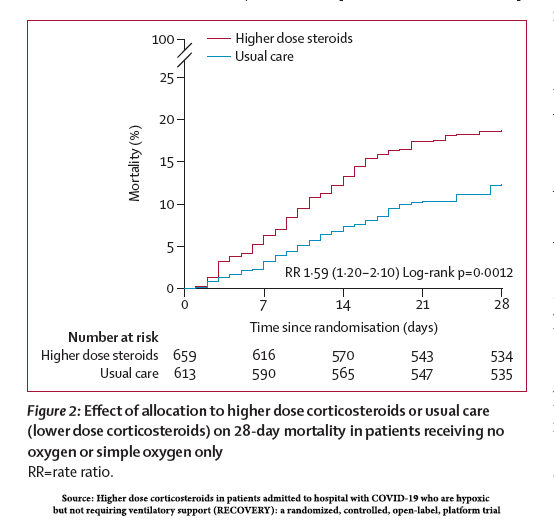
- There were 1,272 patients, 75% of the overall enrollment during the interval, receiving no or little oxygen; 659 randomly assigned to a higher dose corticosteroid, 613 to standard (low-dose corticosteroid) care
 The high-dose steroid group was about two years younger than the mean of 61. Both groups reflected populations from Asia, the UK, and Africa.
The high-dose steroid group was about two years younger than the mean of 61. Both groups reflected populations from Asia, the UK, and Africa.- “Use of other treatments for COVID-19 was broadly similar among patients allocated higher dose corticosteroids and among those allocated usual care.”
Nineteen percent of those treated with high-dose corticosteroids died, compared with 12% in the low-dose group – a 60% increase in mortality risk.
Three-quarters (75%) of deaths were attributable to COVID pneumonia. The heightened mortality was in part due to an absolute increase in the risk of non-COVID pneumonia of 3.7% (relative risk of 40%), a more significant progression to invasive mechanical respiratory support (ventilators), and episodes of high blood sugar (absolute risk increase 7.4%), hyperglycemia, requiring insulin therapy. Elevation of blood sugar is a recognized effect of steroids, but the analysis did not indicate that the increase in mortality was related to diabetes. [2]
The Dose is the Poison
There is still much to be learned from COVID; our experience in the pandemic informs our treatment decisions. Several trials have established the benefit of corticosteroids in managing hospitalized patients with COVID. In this study, patients requiring invasive mechanical ventilation experienced a 33% decrease in mortality. Meta-analysis seems to suggest that acute respiratory distress from whatever microbial cause was improved by steroids. Today’s clinical lesson is that steroids are not for everyone, and more, as with poisons, is not necessarily better.
"The results we present in this Article show that in patients with COVID-19 and hypoxia who require only simply oxygen therapy, a higher dose of corticosteroids …is harmful compared with usual care (which included use of low-dose corticosteroids).”
Do No Harm
For those among us with trust issues, look at how a well-organized clinical study identified and acted quickly to stop the harm. The editorial accompanying the study raises concerns over the underlying causes of the higher mortality and hopes for greater transparency in the data monitoring committee’s deliberations but does not question their responsibility and ability to make that judgment.
This is an excellent example of the self-correcting nature of scientific investigation and may serve as an antidote to the belief that all scientific endeavor is driven by bias and undue influences. This is not a flip-flop but a dynamic judgment based on the evidence. Ask yourself this, when was the last time a politician or a media talking-head said they were wrong, we are stopping what we do? That is why science, although entangled in human behavior, which we often call politics, is sometimes flawed but always strives to reflect our experience of the world.
[1] Among other medications evaluated were hydroxychloroquine, convalescent plasma, and aspirin.
[2] The presence of an underlying co-existent infection at the time of enrollment was physician determined, but as the researchers point out, “the increase in mortality … was similar among patients from the UK and from Asia, suggesting it is not limited to areas with a high prevalence of tuberculosis.”
Source: Higher dose corticosteroids in patients admitted to hospital with COVID-19 who are hypoxic but not requiring ventilatory support (RECOVERY): a randomized, controlled, open-label, platform trial Lancet DOI: 10.1016/S0140-6736(23)00510-X

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


