
In May 2021, a survey conducted by the Robert Wood Johnson Foundation and Harvard T.H. Chan School of Public Health revealed that Americans were rapidly losing trust in public health institutions, most notably the Centers for Disease Control and Prevention (CDC). The decline was driven by the public health agency's recent decision to turn its expertise to solving contentious political issues including racism, gun violence and climate change.
As I wrote at the time, Only 43, 40 and 33 percent of Americans, respectively, said public health agencies should tackle those three issues. “Importantly, unlike public health experts,” the survey reported, “a majority of the public does not currently identify three major problems facing society — climate change, gun violence, and racism — as main responsibilities for public health agencies to handle.”
This should have been a wake-up call to the CDC: Americans don’t want you meddling in contentious political debates. Three years later, it’s clear the agency didn’t get the message. The section of CDC's website dedicated to health equity considerations in infant nutrition now includes this summary:
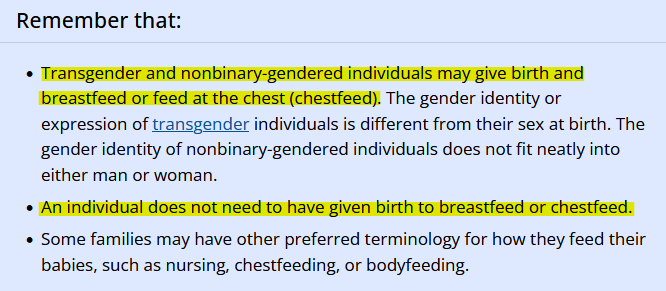
Put another way, the world’s leading public health institution now says that men can give birth and breastfeed should they choose to do so. Not only has the CDC further inserted itself into the culture war, it has done so with almost no scientific justification and at the risk of harming the most vulnerable of all Americans—newborns and infants.
The “science” of breastfeeding
Everybody understood until just a few years ago that women generally begin producing milk during pregnancy, “when hormonal changes signal the mammary glands to make milk in preparation for the birth of your baby,” the Cleveland Clinic notes. Today, though, it’s fashionable to claim that almost anybody can lactate and breastfeed. In fact, “it’s possible to induce lactation in men and in non-pregnant women using the right hormone medications,” the Clinic adds.
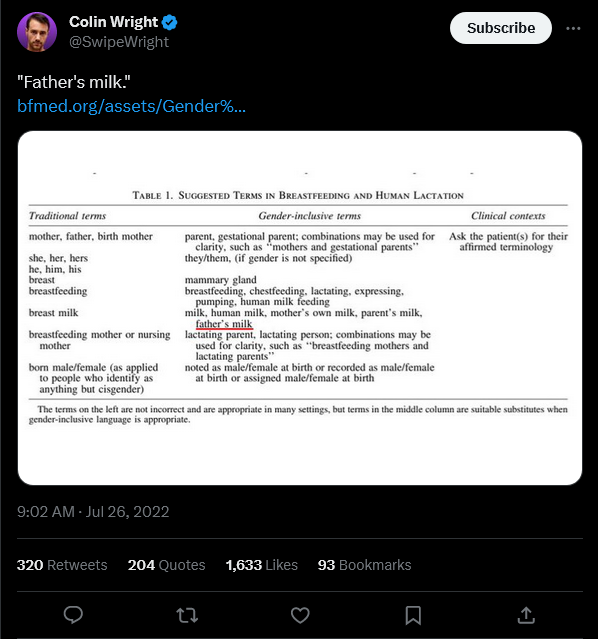
There are some circumstances where lactation apart from pregnancy “might be possible,” according to the Mayo Clinic, for instance, when a woman adopts a newborn and wants to breastfeed. But evidence that men can produce a suitable milk supply to nourish an infant—what the Academy of Breastfeeding Medicine (ABM) calls "father's milk"—is rather scant. That's because the proposition itself is absurd.
This is clear from the November 2020 ABM guidance document CDC cited in support of its recommendations (AMAB below stands for “assigned male at birth”):
“There are many anecdotal reports and one case report of a trans woman (AMAB, on hormone replacement therapy) successfully inducing lactation. Regarding induced lactation in LGBTQ+ parents, we recommend the following based on our experience and the limited published information …” [my emphasis]
The single case report describes a biological male whose female partner didn’t want to breastfeed. After three months of treatment with the hormones estradiol and progesterone and a drug called domperidone, just two weeks before the baby’s due date, this trans individual was producing eight ounces of breastmilk per day. After six weeks of exclusive breastfeeding, “the patient began supplementing with 4–8 oz of Similac brand formula daily due to concerns about insufficient milk volume,” the case report added.
The authors stressed that both the patient and the baby were healthy approximately six months later, but the discussion section of their report outlined some alarming concerns. First, domperidone, an antiemetic used off-label in this case to boost production of the hormone prolactin, is not recommended as a first-line therapy, according to the American College of Obstetricians and Gynecologists (ACOG):
Pharmaceutical galactagogues include domperidone and metoclopramide ... Galactagogues should not be considered as first-line therapy because current research on the effectiveness of pharmaceutical and herbal galactagogues is relatively inconclusive ...
The FDA also banned the drug in 2004, as the case report explained:
“Domperidone is not currently available in the United States for gastrointestinal use due to the FDA's concern about its association with cardiac arrhythmias, cardiac arrest, and sudden death when used intravenously. The FDA has warned against domperidone's off-label use as a galactogogue due to its unknown risks on breastfeeding infants.” [my emphasis]
What about "endocrine disruption"?
A similar issue affects trans men (biological women) who get pregnant while they are transitioning. Testosterone therapy is a routine part of that process, and most health care providers have urged these patients to stop taking the hormone while pregnant because of risks to the child. In an article meant to justify testosterone therapy during pregnancy, The Conversation unintentionally let slip just how groundless that practice is:
The health care providers we interviewed expressed concerns about patients continuing testosterone while pregnant or chestfeeding. When we asked them what risks they were most concerned about, they often noted that there is either not enough or inconclusive research on using supplemental testosterone during pregnancy. Despite this, nearly all of the providers we interviewed routinely advised patients to pause testosterone therapy without reservation. [my emphasis]
The harms to the child in this situation are potentially very serious. Again, according to The Conversation, they may include a higher risk of “the baby later developing intersex conditions, or having biological traits that do not fit binary definitions of male or female characteristics … metabolic and cardiovascular dysfunction, such as obesity; and neuropsychiatric disorders, such as autism and attention-deficit disorder.”
The Conversation’s only rebuttal to these concerns expressed by physicians was to say that their “focus on producing ‘normal’ children fails to attend to both natural human diversity ... and the mental health of trans and nonbinary parents ... It may also echo eugenicist policies that attempt to eliminate human characteristics and communities that society deems inferior or bad.”
Not only is that response dismissive of legitimate concerns about how testosterone therapy may harm children, it comes from a website that has bought into the hysteria surrounding endocrine (hormone)-disrupting chemicals.
Just last week, in fact, The Conversation published an article alerting young women that their beauty products may contain "... endocrine-disrupting chemicals that can interfere with fertility and reproduction, fetal growth and infant development." The CDC has also expressed the same concerns about so-called "endocrine disrupting chemicals found in the environment," including certain pesticides and industrial chemicals.
In sum, exposure to trace amounts of thoroughly tested chemicals approved for use in consumer and industrial products could harm your children. But exposing them to supplemental testosterone in utero is an acceptable risk if you're transitioning genders. Never mind the blatant contradiction, citizen! Social justice must prevail!
Worth the risk?
All medical interventions carry some risk. So, someone will no doubt object to my argument, perhaps using domperidone and other drugs is worth the risk if it allows trans men and women to give birth and breastfeed. While that perspective may seem reasonable to some, it’s again hampered by a dearth of evidence. The “transgender revolution,” as it’s sometimes called, is less than a decade old, and that means we know next to nothing about milk production in trans people receiving gender-affirming care.
Moreover, we may never be able to produce the rigorous evidence regulators and patients usually expect for other interventions given the small population of breastfeeding trans men and women. As the 2020 ABM guidance document concluded:
"Significant research gaps exist in this field. In the future, it is unlikely that grouping sexual orientation and gender identity will provide appropriate research or practical guidance … community-based participatory research and qualitative studies informing future research and support should be strongly considered."
Qualitative research has a legitimate place in science, but as the National Institutes of Health (NIH) says, “It answers the hows and whys instead of how many or how much.” Key questions about the safety and efficacy of the different drugs used in these cases—how much and how many—can’t be answered with qualitative study designs because the data they produce “can be observed, but not measured,” NIH notes elsewhere.
Conclusion
If you ask a journalist or fact-checker why "misinformation" is such a widespread problem today, they'll almost certainly lay the blame on Robert F. Kennedy, Jr. or some other high-profile iconoclast with a lawsuit to file or a supplement to sell. And with good reason. Kennedy and his allies are deeply confused activists; their conspiratorial claims about vaccines, pesticides and GMOs are flatly contradicted by a wealth of evidence.
That said, before NBC or the New York Times churns out yet another listicle about Kennedy's "5 noteworthy falsehoods," perhaps one of these esteemed news outlets will grill the CDC for telling men they can grow breasts and produce milk to feed infants. I'm not hopeful given the media's track record, though maybe things will be different this time.
The reality is that this little scandal has amplified one of the fundamental issues plaguing our discussions about so many science and health issues: CDC (and EPA and FDA) officials, like so many other experts, will happily spread nonsense if it conforms to fashionable political ideas.

Cameron English
Executive Vice President
Cameron English is a writer, editor and co-host of the Science Facts and Fallacies Podcast. Before joining ACSH, he was managing editor at the Genetic Literacy Project.


