
The study, reported in the American Journal of Medicine (AJM), is a meta-analysis of articles posted in “the voice of the CDC,” its weekly Morbidity and Mortality Weekly Report (MMWR). The indictment being made is that for the MMWR reports:
“... our findings highlight the journal’s lack of reliance on high-quality data and a tendency to make strong but unsupported causal conclusions about mask effectiveness.”
“high-quality data”
The authors begin to construct their straw man [1] almost immediately.
“MMWR is a weekly scientific journal without external peer review overseen by the CDC to publish data on nationally notifiable infectious diseases, which can then be used for program planning, evaluation, and policy development.”
The authors then describe their search for “MMWR face mask studies.” The straw man is now fully constructed, the (false) conceit that their meta-analysis considers studies in a weekly scientific journal.
While it is true that it publishes data, MMWR is certainly not a journal, digital or print – the most commonly considered definition of a journal requires peer review. The authors forgot to include this, also from the CDC’s official documentation:
“The data in the weekly MMWR are provisional, based on weekly reports to CDC by state health departments.” [Emphasis added]
While these reports are indeed studies, they are wholly observational reports of data collected by state agencies – they are not pre-specified clinical trials. Because they are observational trials
“researchers are looking at the effect of some type of intervention, risk, a diagnostic test or treatment, without trying to manipulate who is, or who isn’t, exposed to it.”
There are no control groups. And because they are reports, there is no need for a protracted discussion that would more formally include a brief review of pertinent literature in the context of the study’s findings.
It is no wonder that among the flaws noted by the authors is a lack of controls, randomization, and discussion of randomized and conflicting data. Of course, these are not flaws at all unless you treat them as peer-reviewed, non-observational studies, which they are not. In the vernacular, the absence of controls is “a feature, not a bug.”
The flaws noted by the authors are depicted in this graphic taken from their meta-analysis. I have highlighted in yellow the only arguments remaining after we recognize that a straw man argument was made.
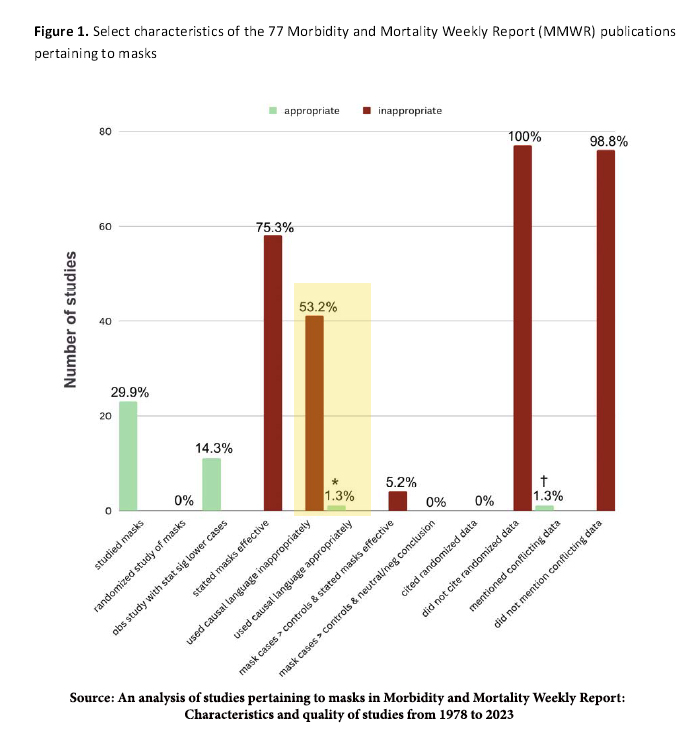
To be fair, an argument can be made that these reports stated that masks were effective, but we must apply two large grains of salt. First, as the authors note, few of the “studies” looked at masks at all. Second, the context of stating masks are effective is not mentioned.
Cherry Picking - “unsupported causal conclusions about mask effectiveness.”
The researchers defined causal language
“as using terms such as, “can,” “likely,” “led to” or otherwise drawing definitive conclusions about mask effectiveness which was not based on references to other studies.”
“Over 50% of the identified studies used causal language in their conclusions about mask effectiveness.”
They are identifying this language in 50% of the studies. Of course, the format of MMWR reports is such that references to other studies aren’t warranted – these are real-time public health investigations or reports. These are raw data points, not clinical trials.
The authors note that the grading of the use of causal language was subjective, quickly adding that those subjective views were arrived at using a “double-blinded system.” They bolstered the “objectivity” of their subjective judgment by citing a kappa statistic, a measure of agreement, as being “substantial.” That should not be difficult; the authors are all members of the same research team – so much for diversity of thought.
What follows are several of the eleven examples offered in the AJM article to demonstrate the use of causal language. The authors’ cherry-picked phrase is in bold, surrounded by the context which makes it clear that these examples are misstatements.
“This investigation highlights a need for prevention strategies focused on enhanced community education related to recognition of COVID-19 symptoms and encouraging consistent mask-wearing. All household members, including the index patient, should wear masks within shared spaces in the household. These strategies, along with self-isolation upon symptom onset, can limit exposures and mitigate transmission.”
“These findings suggest that transmission of SARS-CoV-2 within households is high, occurs quickly, and can originate from both children and adults. Prompt adoption of disease control measures, including self-isolating at home, appropriate self-quarantine of household contacts, and all household members wearing a mask in shared spaces, can reduce the probability of household transmission.”
“The Lake County Health Department (LCHD) in Illinois introduced a Test to Stay (TTS) strategy, whereby unvaccinated students, teachers, and staff members with certain school-related COVID-19 exposures could remain in school and participate in school-related extracurricular activities. Eligibility to participate in TTS required the following conditions to be met: 1) the exposure occurred while both the person with COVID-19 (index patient) and the close contact were masked; 2) the close contact remained asymptomatic, practiced consistent mask wearing, and maintained physical distancing; and 3) the close contact underwent testing for SARS-CoV-2 (the virus that causes COVID-19) on days 1, 3, 5, and 7 after exposure to the index patient.
Although vaccination remains the leading public health recommendation to protect against COVID-19 for those aged ≥5 years, schools might consider TTS as an option for allowing close contacts who are not fully vaccinated to remain in the classroom as an alternative to home quarantine.
Implementation of a TTS strategy with multiple prevention components, including masking and physical distancing, resulted in low secondary transmission of SARS-CoV-2 in K–12 schools in Lake County, Illinois.”
Finally, this snippet of a more extended discussion.
“However, even if a person is infectious after an initial diagnosis, the risk for transmission to others depends on other important factors, including the duration and proximity of contact with others, and proper use of a well-fitting mask. Following CDC recommendations,§§ YKHC advised continued mask use for 10 days after symptom onset even if a person met the criteria for ending isolation after 5 days. The high percentage of positive antigen test results during the 5–9 days after symptom onset reinforces the importance of correct and consistent mask use during this period.”
In the presence of ongoing infection, masks, in addition to other behaviors, is important. Where are the causal words?
Words and Deeds
The CDC, along with other federal agencies and a plethora of experts, made mistakes, especially concerning communication during the Pandemic. This most recent AJM study does little to understand how we might do better; it provides fodder for divisive, not diverse, views.
“When an issue is deeply polarizing, publishing bad science helps no one. It cannot convince skeptics, proponents don’t need convincing, and it deepens mistrust in institutions.” – Vinay Prasad, MD MPH
As a clinician, I believe masks have value. I am not alone in that belief here at ACSH, as discussed by my colleague, Dr. Henry Miller, or in the larger medical community. The senior author of this study is a well-known social media expert and practicing oncologist, Dr. Vinay Prasad.
Let’s cut through all the rhetoric and ask Dr. Prasad about his words or deeds. What do you recommend for your immunocompromised patients concerning masking? The institution where you practice medicine in their September 2023 guidance states:
“To keep everyone safe, masking is still required for all patients, staff and visitors in all areas where patients are present.”
Are you compliant with those rules? Have you, as a member of the medical staff, indicated your strong belief to the hospital administration that this causal statement has no foundation?
[1] A straw man argument is an intentional misrepresentation set up because it is easier to defeat in an argument than the opponent's real argument.
Source: An analysis of studies pertaining to masks in Morbidity and Mortality Weekly Report: Characteristics and quality of studies from 1978 to 2023 American Journal of Medicine DOI: 10.1016/j.amjmed.2023.08.026

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


