
Prostate cancer is a much-discussed form of cancer in the medical literature. In part because of its sheer impact on all men but also because of the disparities in assessment, treatment, and outcome often couched along the lines of that social construct, race. Prostate cancer, given its recurrent prominence in our news cycles of late, may be a helpful way to begin to disentangle social determinants and genetics when we insist on discussing a disease stratified by race.
Some Context
- Prostate cancer is the second leading cause of cancer-related mortality in men, following only lung cancer.
- The incidence is low in Asian men, higher in Northern Europeans, and highest in African-American men. In the US, the incidence is 64% greater in African-American men than Whites
- In the US, mortality from prostate cancer in African American men is twice that of Whites and 3 to four-fold greater than Asians,
- “Black men experience higher prostate cancer incidence, earlier age of diagnosis, more advanced disease at diagnosis, poorer access to diagnostics and treatments, and ultimately, worse outcomes.”
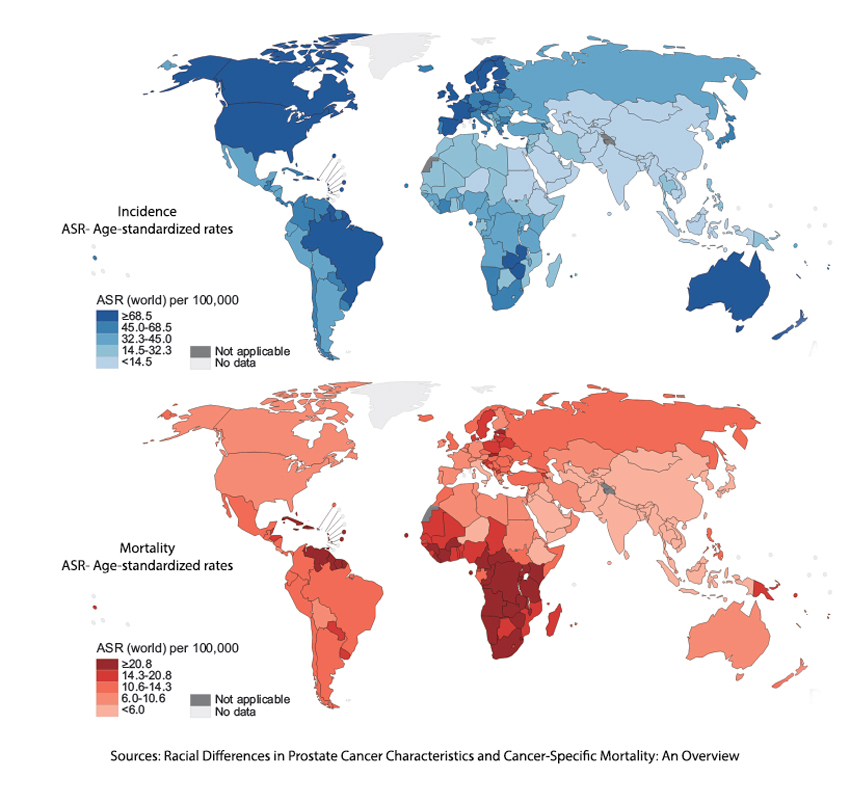 Focus for a moment on the graph demonstrating the global incidence and mortality of prostate cancer and how the US incidence is nearly five-fold greater than that in Africa. Our mortality is half that of Africa, so diagnostic evaluation and treatment outcomes are entangled with race and socioeconomic factors.
Focus for a moment on the graph demonstrating the global incidence and mortality of prostate cancer and how the US incidence is nearly five-fold greater than that in Africa. Our mortality is half that of Africa, so diagnostic evaluation and treatment outcomes are entangled with race and socioeconomic factors.
Screening
The days of a rectal examination for prostate cancer are quickly coming to an end as the more accurate and less feared blood test for the Prostate Specific Antigen (PSA) supplants it. As with all screening tests, PSA comes with an increased risk of a false positive, leading to more anxiety, invasive testing, and cost. The US Preventative Services Task Force (USPSTF) guidelines revised as recently as 2018 recommended against PSA screening in those men younger than 55 and individual decision-making for those older until the age of 70 when they believed no further testing was warranted.
However, the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) registry demonstrates that Black men experience prostate cancer anywhere from 1.2 to 3 years earlier than White men. More importantly, given all the concern about the misuse of “race” in clinical testing, e.g., kidney function measured by serum creatinine, studies done by the VA demonstrate that the PSA level cut-off of 2.5 is too high for Blacks, and when that is taken into account a lower value, 1.9, is a more sensitive marker of active prostate cancer.
Bottom line. We under-screen for prostate cancer in African American men. As a result, along with a general reluctance by men to be screened [1], African American men are diagnosed at a later stage of disease.
Treatment
There is a wide range of treatment options for men based on the extent of prostate cancer, as measured in the past by CT scans and, more recently, by MRI scans that are better at detecting changes in the soft tissues. In addition, a biopsy of the tumor is performed, and the aggressiveness of the tumor is graded using what is called a Gleason Score. The means of guiding the biopsy has also changed over time, going from blind “stabs” into the prostate to more guided attempts using ultrasound and MRI.
Active surveillance is a frequent option when the tumor is less aggressive, with a Gleason Score of 6 or less, and contained. It requires routine annual follow-up. Over time, Black men are choosing that option less frequently, opting instead for surgical, chemical, or radioactive interventions. A study in the NEJM using 2015 SEER data demonstrated that when only considering race, the odds ratio of a black man choosing active surveillance was 0.94. When adjusting for socioeconomic determinants of health, including insurance type, the odds ratio of choosing active surveillance rose to be comparable with other races, 1.06. [2]
Biological Disparities
Race is a poor marker of our biological underpinnings; skin color has no value. To understand biological mechanisms, we need genetic ancestry data, which is in short supply. But we can make some generalizations.
- Black patients are more likely to harbor DNA repair mutations of any kind.
- Androgen receptors (AR) play a central role in the development and functionality of the normal prostate and the initiation and progression of prostate cancer. AR mutations are rare but more prevalent in Black patients than the others, and those mutations are associated with more aggressive tumor behavior.
- A high-fat diet and obesity are strongly linked to the incidence and progression of prostate cancer. Rapidly proliferating cancer cells enhance de novo lipogenesis to support their growth. Black men with prostate cancer exhibit elevated expression of crucial de novo lipogenesis genes, indicating a potential association with tumor aggressiveness and poor clinical outcomes.
Prostate Cancer and Socio-economic Determinants
A study of California’s Cancer Registry looked at, among others, 270,000 first diagnosed with prostate cancer between 2000 and 2013. The researchers using mediation analysis identified the following factors contributing to disparities in prostate cancer health outcomes. (You can find more about the technique and its impact on the evaluation of prostate cancer here.)
- 24% of the disparity in survival was attributable to the stage at the time of diagnosis – where the absence and application of more personalized guidelines could improve outcomes
- 14% was attributable to marital status – where a wife pushed the reluctant into getting care
- 7% due to neighborhood socioeconomic determinants of health – where the lack of resources, often financial or related to health literacy, and the presence of “stress” may play a role.
When all of these factors were adjusted,
“the survival disparity between black and [Non-Hispanic White] men with prostate cancer [was reduced] to nonsignificant levels.”
Other factors that include the underlying differences in biology, whether evolved or expressed as a condition of their current environment, explained 52% of the variance.
[1] “Men are willing to participate in prostate cancer screening to prevent cancer and gain reassurance about their health, particularly when supported or prompted by their social networks or healthcare providers. However, to do so, they needed to mentally overcome fears of losing their masculinity and accept the intrusiveness of screening, the ambiguities about the necessity, and the potential for substantial costs.”
[2] It is the difference between 0.94 and 1.06, 12%; some would consider that to reflect “structural racism” in healthcare. I would suggest that it reflects caste.
Sources: Racial Differences in Prostate Cancer Characteristics and Cancer-Specific Mortality: An Overview World Journal of Men’s Health DOI: 10.5534/wjmh.210070
Racial disparities in prostate cancer: A complex interplay between socioeconomic inequities and genomics Cancer Letter DOI: 10.1016/j.canlet.2022.01.028
Racial and Ethnic Disparities in Cancer Survival: The Contribution of Tumor, Sociodemographic, Institutional, and Neighborhood Characteristics Journal of Clinical Oncology DOI: 10.1200/JCO.2017.74.2049

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.



{kind=link}