
Prostate Cancer – Diagnosis and Staging
Before considering the study, we need some context. Prostate-Specific Antigen (PSA) is a biomarker of cancer identified from a simple blood test. As men age, our PSA rises, but reasonably clear points indicate that the rise is “abnormal” and suggests that prostate cancer might be present. The definitive test is a prostate biopsy which can “almost” accurately determine the presence of prostate cancer. Because some biopsies are “blind,” done without guidance by imaging, some areas of the prostate may not be biopsied, and a cancer is missed.

In those patients with biopsy-proven cancer, determining the extent and the aggressiveness of the cancer is the next important step – it is referred to as "staging."
The biopsies provide the physician with a Gleason score – a determination from looking at the cellular architecture of how poorly differentiated the cells are from normal. The more poorly differentiated, the more aggressive the tumor may be, i.e., likely to spread and metastasize. The second part of staging is to search for cancer that is outside the prostate, has it already spread to the surrounding tissue or lymph nodes. Staging guides treatment choice from observation to surgery, radiotherapy, or chemotherapy.
The Study
The researchers used a dataset combining Medicare data with that of SEER - Surveillance, Epidemiology, and End Results Program of the National Cancer Institute. SEER captures data from many of the cancer registries nationally. The researchers want to determine the racial disparity in the use of MRIs in the staging of prostate cancer. To that end, they sought all patients over age 66 with
“a diagnosis of clinically localized (i.e., nonmetastatic and lymph node-negative) prostate cancer between January 1, 2011, and December 31, 2015.”
There is a problem with this definition. How would they know that the disease was “clinically localized” without an MRI? Perhaps they had a CT scan, which would have provided similar information. [2] But without additional information, we do not know much more about their “staging” than their Gleason scores.
They identified 39,534 eligible patients
- 3,979 (10%) Black, 251 (6.3%) had an MRI
- 32,585 (82%) White, 3,216 (9.8%) had an MRI
- 2,970 (7%) of other races, 284 (9.5%) had an MRI
- There is no disparity between the rates of MRI for Whites and “other races.”
- A Black male is 33% less likely to have an MRI than a White Male
The first thing you should recognize is that 90% or more of men did not have any staging by imaging at all in every instance. Why would this be? Are physicians acting outside the standard of care 90% of the time? The answer here requires two more pieces of clinical expertise. Prostate cancer is generally a slow-growing tumor, something you can “live with.” Because it is slow-growing, treatment may be a “cure greater than the disease.”
“The recent National Comprehensive Cancer Network (NCCN) guidelines list active surveillance as an initial therapy option for men with favorable intermediate-risk disease, which they define as clinical stage T2b-T2c, Gleason score 3+4, or prostate-specific antigen (PSA) levels at 10–20 ng/mL, as well as less than 50% of positive biopsy cores.”
Active surveillance, watchful waiting, remains controversial for higher Gleason scores but is increasingly the standard of care for low-risk cancers. [3] The researchers noted that the disparity in MRIs between Blacks and Whites, when adjusted for “lower clinical risk,” was 10-fold less, 3%.
Using a technique called mediation analysis, the researchers drew additional conclusions. Unfortunately, this will also require a bit of explanation.
Mediation Analysis
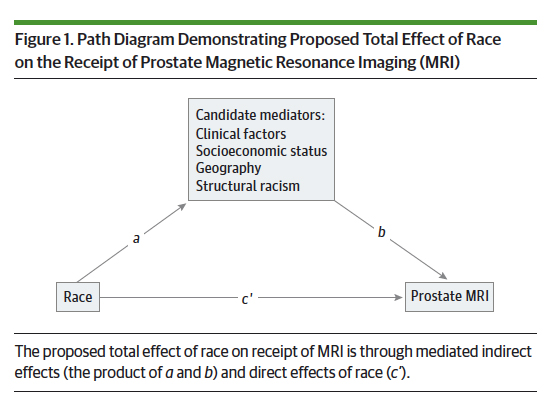 This diagram should help. Most studies looking at the effect of race on prostate MRI would suggest a direct association, line c’. Mediation analysis proposes an additional indirect association through intermediary or mediator variables that impact the outcome. In this study, clinical factors, socioeconomic status, geography, and structural racism all are affected by race, line a; and subsequently mediate (modify) the outcome, line b, the performance of a prostate MRI.
This diagram should help. Most studies looking at the effect of race on prostate MRI would suggest a direct association, line c’. Mediation analysis proposes an additional indirect association through intermediary or mediator variables that impact the outcome. In this study, clinical factors, socioeconomic status, geography, and structural racism all are affected by race, line a; and subsequently mediate (modify) the outcome, line b, the performance of a prostate MRI.
All of these associations, direct and indirect, are measured using logistic regressions, where the impact of a given variable is given by its coefficient. For a direct variable (race), the bigger the coefficient, the larger the effect. In mediation analysis, attention is not paid to the size of the direct variable’s coefficient but to how it changes with the addition of the mediators. The degree to which the coefficient is reduced, if at all, measures the mediator’s effect. [4]
The researcher’s concern was which mediators exerted the most substantial influence.
“In this population-based cohort study of US adults, using mediation analysis, sociodemographic factors, including geographic variation, poverty, and structural racism, explain most of the observed racial disparity in prostate MRI use among Black and White Medicare beneficiaries with a new diagnosis of prostate cancer.”
Here is the data;
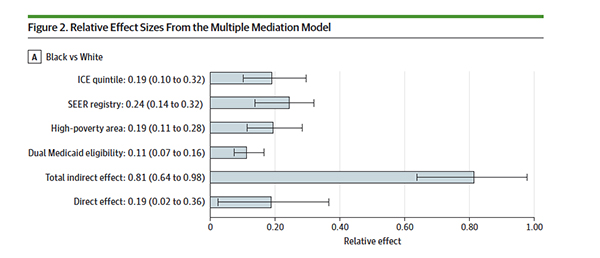
- The direct effect of race accounted for 19% of the disparity
- 24% was due to differences in MRI usage regionally
- 19% was due to living in an area of “high-poverty.” [4]
- 19% were due to high levels of segregation (ICE quintiles) [5]
- 11% were due to dual Medicaid eligibility – another marker of poverty
The most significant mediator was to what degree MRI was used in your region, not your zip code or census tract. Your regional physicians' “standard of care” was the most significant factor. It was greater than poverty, segregation, or race; only when combined as “structural racism” did it easily surpass the standard of care.
“The model that we constructed is inherently constrained by the candidate mediators that were selected for this retrospective analysis.”
Among the candidate mediators are clinical factors, namely the Gleason scores. But somehow, their impact doesn’t make it into Figure 2. Where did the mediation effect of the clinical factors go - we already know that adjusting for them reduced the disparity to 3%.
I do not doubt that structural racism is real, providing a historical explanation for residential segregation and poverty. Race is more than a social construct; there is a biological heritage. Black as a racial category is far too broad and doesn’t consider any ancestorial differences among those born in the Caribbean, the West, or East of Africa. It is no different than the exceedingly broad brush of the term White, which includes more the Anglo-Saxons.
This study points at a problem, offering a new statistical lens, mediation analysis, to search for a cause. But the absence of clinical data makes it far from the perfect study, especially given that the researchers had the Gleason scores. “Perfection is the enemy of good,” but this study is too easily dismissed as clinically irrelevant – it does not, to my mind, serve the cause of health equity well.
[2] MRI is a better modality than CT because it detects soft tissue changes, like growth outside the prostate better.
[3] Some patients are quite content to watch and wait; others, once they hear the term cancer, want it treated irrespective of the physical costs; the mental price of observation is too great.
[4] >20% of census tract living below poverty levels
[5] Based on the ratio of Blacks to Whites in a given census tract – higher scores “greater degrees of racialized residential segregation.”
Source: Mediators of Racial Disparity in the Use of Prostate Magnetic Resonance Imaging Among Patients With Prostate Cancer JAMA Oncology DOI: 10.1001/jamaoncol.2021.8116

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


