
In plain language, “food is medicine” programs provide free, healthy food through clinical care to patients whose conditions may be affected by diet and who also struggle to afford enough food.
What Are Medically Tailored Meals?
Medically tailored meals (MTM) are designed by a nutritionist for individuals with “diet-sensitive” (i.e., metabolic) disorders, including cardiovascular disease, diabetes, and renal insufficiency (where dietary restriction slows disease progression), and are then delivered – you might think of it as a mash-up of a nutritionist, SNAP, and HelloFresh. Several states have federal waivers to test these meals as a Medicaid preventive. Nature Medicine has a report on how it is going in Massachusetts.
The Massachusetts Experiment
In the Massachusetts demonstration, roughly 1,800 Medicaid patients received five lunches, five dinners, and snacks each week for about six months. All were members of Medicaid Accountable Care Organizations, health care groups paid to coordinate care and manage costs. After a nutritional assessment, participants received meals tailored to their medical needs, with 15 meal plans available. The meals were intended for the patient alone, not for other family members—a detail that matters when considering food insecurity at the household level. Researchers then tracked primary care visits, emergency department visits, hospitalizations, and associated costs.
Promising Results
The meal participants' outcomes were matched with those of similar members of the Medicaid ACOs. During the six months of MTM delivery, the MTM recipients had a
- 31% lower rate of hospitalization
- 20% lower rate of ED visits
- No significant change in primary care visits
- $3,433 lower health care costs [1]
than their matched peers.
And now, the Caveats
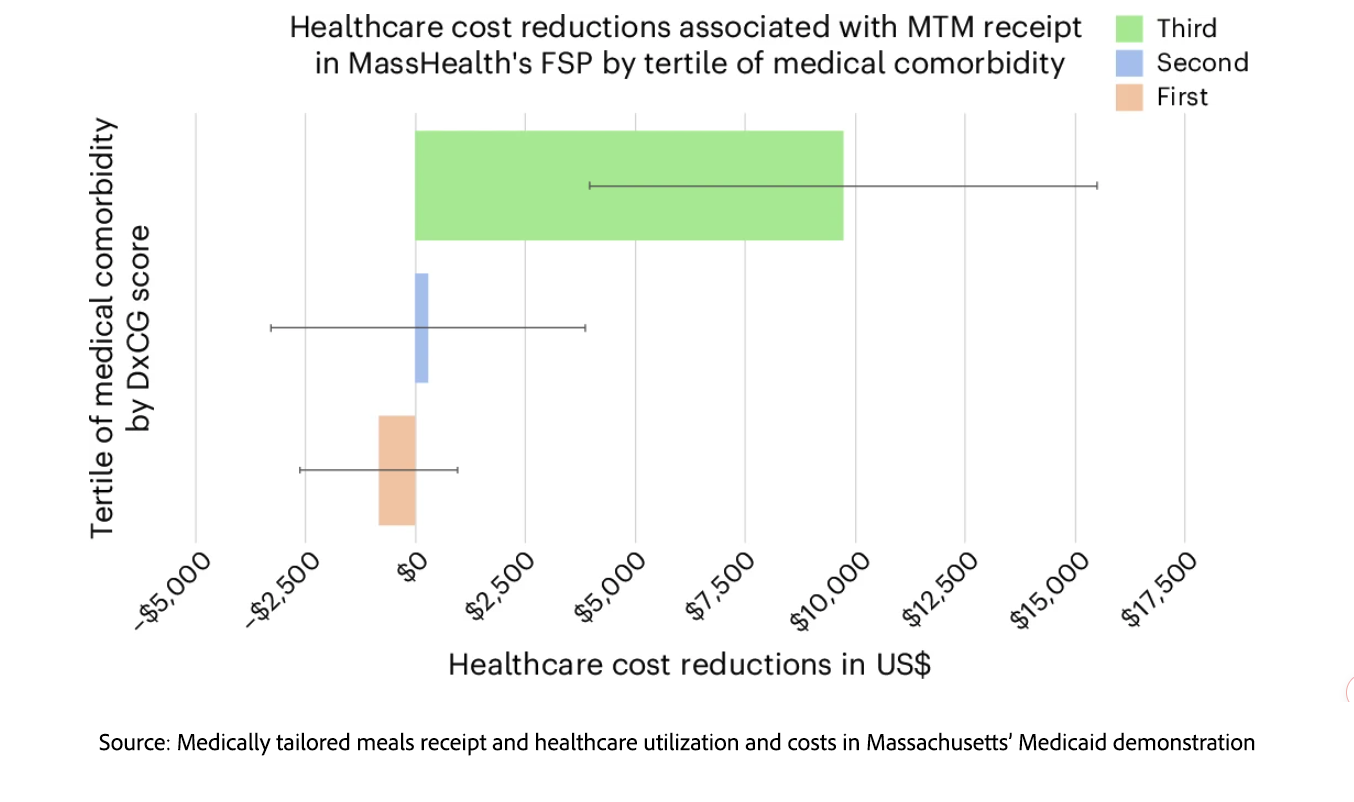
The cost savings were concentrated among patients with the greatest number of comorbidities. For participants with fewer underlying medical problems, medically tailored meals appeared to increase total spending rather than reduce it. That distinction matters because it suggests that medically tailored meals may work best not as a broad Medicaid cost-saver, but as a targeted intervention for patients at highest medical risk.
Give a Man a Fish, or Teach Him to Eat Better?
The savings also disappeared among participants who left the program before six months, raising questions about engagement, continuity, and who is most likely to benefit. Participants were offered optional nutrition counseling and training, but 62% attended none of the three classes, while only 5% attended all three. That may suggest that the delivered food was the stronger draw. But low attendance could also reflect practical barriers—work schedules, transportation, caregiving demands, illness, or limited trust in health care programs. In a food-insecure household, the value of delivered meals may also extend beyond the patient, even if the meals were officially intended for that person alone.
Lower health care utilization and cost savings were evident within the cohort when stratified by disease, with the greatest reductions for cardiovascular and renal disease, both of which have strong dietary treatment components. This pattern also held for depression and anxiety, where diet is not considered a significant disease driver, and may again reflect the value of food for the food-insecure in reducing stress.
Finally, the researchers had no way to confirm meal adherence because they lacked dietary data. That limitation matters. Without knowing whether participants ate the meals, shared them, supplemented them, or changed their overall diet, we cannot determine whether the apparent benefits stemmed from improved nutrition, reduced food insecurity, increased contact with care systems, or a combination of these. Nor do we know whether any benefits persisted after the meals stopped arriving.
Food as Medicine — or Food as Food?
The Massachusetts MTM demonstration is intuitively appealing, feeding people who are both sick and food insecure appears to reduce acute medical utilization while they are receiving meals. These results support the common-sense proposition that food can be a stabilizing intervention for vulnerable patients, and may produce short-term benefits that matter to patients, providers, and payers alike.
Yet because of the study’s limitations, especially not determining whether participants ate the meals, we cannot say whether improved nutrition or some other mechanisms, such as reduced financial stress, drove their results. Importantly, it cannot tell us whether medically tailored meals produce lasting improvements in health once the food stops arriving.
The generous interpretation is that food assistance, when targeted to medically fragile and food-insecure patients, can act as a practical medical intervention. If the goal is to reduce short-term hospital use among high-cost Medicaid patients, the study provides encouraging evidence for a useful clinical adjunct for selected patients. The more skeptical interpretation is that “food is medicine” may be less a new therapeutic category than a medicalized pathway for delivering food aid to people in need. Much of the apparent benefit may come from meeting a basic human need that the healthcare system has inherited because other social systems have failed to meet it.
[1] After accounting for meal costs, the program nearly broke even during the active delivery period, with a net cost of $14.90 per person per month.
Source: Medically tailored meals receipt and healthcare utilization and costs in Massachusetts’ Medicaid demonstration Nature Medicine DOI: 10.1038/s41591-026-04407-5

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


