A recent article in the NY Times informs readers that researchers have identified a set of proteins that can predict lung cancer five years before they become symptomatic and that an anti-inflammatory drug “could significantly reduce lung cancer risk in people with elevated concentrations of these proteins.”
This sounds almost too good to be true. Is it?
The underlying study was published in the journal “Cell”. It details results from a complex, multifaceted BioBank research project that provides investigators with new information on how lung cancers and lung carcinogenesis might be driven by a combination of molecular changes from smoking and lung inflammation. While I am not qualified to assess whether the article’s conclusions on lung cancer’s molecular carcinogenesis are correct, I have been repeatedly disappointed by new claims that blood tests can detect early-stage cancers before symptoms appear, only for those claims to later fail. In a recent study, Grail’s Galleri test failed. Is the Cell study another example?
Experimental Findings
Most often, we determine high risk of lung cancer from clinical parameters, i.e., the patient’s age, smoking history, family history, etc. The authors found no greater “predictability” in their 14-protein “signature” than clinical findings when each was considered separately; however, when combined, the information they augment one another. This is reflected in the graph demonstrating the area under the curve (AUC) [1] from both the clinical model and blood test.
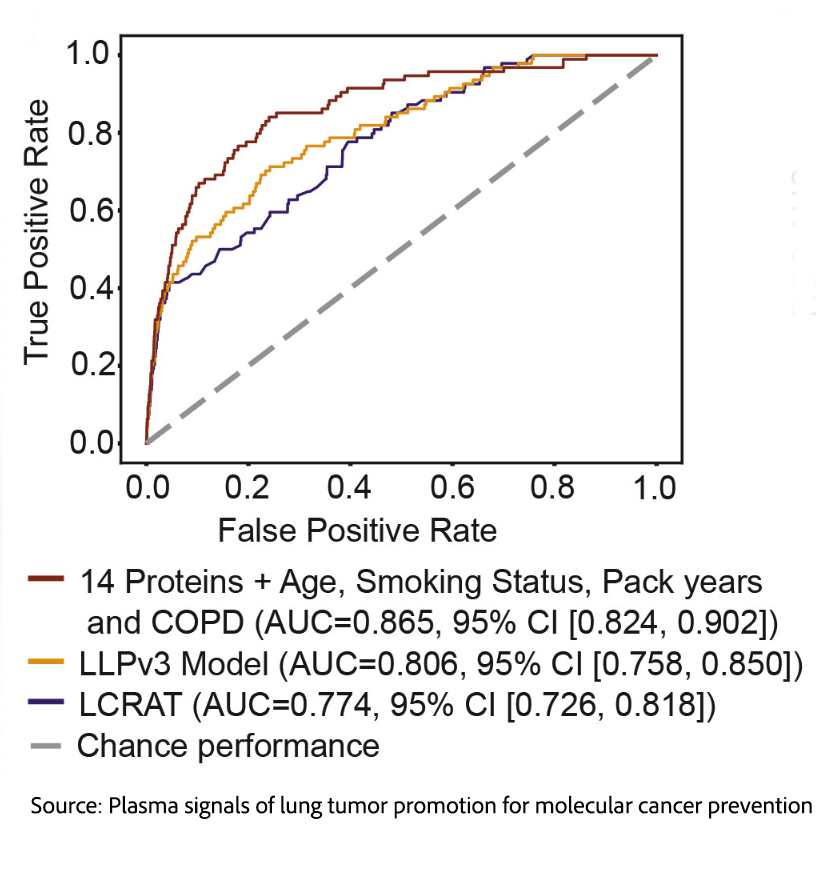
The AUC for the usual risk factors was 0.806, while the AUC when the protein signature was added rose to 0.865.
Put more simply, using the protein signature improved the ability to predict future lung cancer by 5%, a small percentage, but even a little bit better is desirable when dealing with a highly lethal cancer.
The authors went on to discuss a clinical trial of an anti-inflammatory drug, canakinumab, an interleukin-1 beta inhibitor, which failed to reduce mortality from cardiac disease in the CANTOS trial. Canakinumab was repurposed as a treatment for lung cancer, where it again failed. However, it was noted to be associated with a lower risk of developing lung cancer.
Reexamination of data from CANTOS suggests that the number of people in the general population who would need to be treated (NNT) with canakinumab to save a life would be more than 1500. However, if the screened population was “enriched” to include only those with both a clinical risk and the protein signature, the NNT might improve to as low as 55. While no experimental chemoprevention has been effective in reducing lung cancer incidence, if canakinumab could be shown to reduce the incidence of lung cancer without significant drug-related morbidity, it might well be prescribed to this high-risk population and prevent many lung cancers.
Challenges in Implementation
Multiple problems remain to be resolved.
The FDA website discloses that canakinumab is a potent immunosuppressant, posing known risks of activation or progression of tuberculosis and other serious infections. Hypersensitivity reactions, including anaphylaxis, have been reported. Most importantly, mortality from infection was significantly higher in the CANTOS canakinumab treatment arm.
Neither the New York Times nor Cell articles addressed the cost of the protein test or of treatment with canakinumab. A commercial test for the 14-protein panel has not yet been developed. Based on the prices of currently available multi-cancer early-detection molecular tests like Galleri, the price would range from $750 to $1000 before any discounts.
Based on an estimated cost of canakinumab, annual preventive treatment would cost over $250,000 and would need to be continued for more than five years.
Ignoring cost and toxicity concerns for the moment, could a trial that randomizes high-risk individuals be completed? Most eligible patients would already be eligible for low-dose CT screening. Would it be ethical to withhold this far more sensitive test, recommended by guidelines and covered by both Medicare and private insurance, from high-risk patients in both the treatment and control arms?
If CT screening were incorporated into the research protocol, the number of research subjects required to reach statistical significance would have to be much larger, increasing the complexity and cost of research.
Future Directions
This study extends our consideration of whether and to what extent blood-based biomarkers may help refine lung cancer risk prediction beyond age and smoking history alone. Unfortunately, the proof of concept is not yet established. The reported improvement in discrimination suggests that molecular screening tools could one day help identify high-risk individuals who might otherwise be missed. That matters because lung cancer outcomes depend heavily on early detection, and better risk stratification could make screening both more precise and more efficient.
However, these findings should be viewed as encouraging rather than definitive. An improved AUC is useful, but it does not, by itself, prove that the test will reduce deaths, avoid unnecessary follow-up, or perform equally well across diverse populations and clinical settings. Before such an approach can be widely adopted, it will need external validation, prospective testing, cost-effectiveness analysis, and careful assessment of false positives, false negatives, and downstream harms.
The ideal is not that biomarkers will replace clinical judgment or existing screening programs, but that they might strengthen them. If validated, protein-based risk models prove their ability to improve outcomes, not just staging, it could help move lung cancer screening from a blunt eligibility framework toward a more individualized, precision, public health strategy. This remains a work in progress.
[1] The AUC measures the ability to discriminate between two categories, in this instance between those at low and high risk. 0.5 is essentially the discrimination of a coin toss; 1 is perfect separation.


