
For patients, alpha-gal syndrome can be startling. A tick bite in the summer can lead, months later, to hives, gastrointestinal distress, or even life-threatening anaphylaxis hours after eating a hamburger or steak. The delayed nature of the reaction makes the condition difficult to recognize and even harder to diagnose.
An Allergy Hidden in Plain Sight
It began with a monoclonal antibody, a laboratory-engineered immune protein designed to treat colorectal and head and neck cancers. Nationally, fewer than 3% of individuals developed severe anaphylactic or urticarial reactions (hives), but 22% of patients in North Carolina and Tennessee developed those complications. An analysis of 25 of those patients found that the majority had hypersensitivity to the monoclonal antibody due to specific IgE.
While the other major antibodies fight infection, IgE triggers our allergic responses by binding tightly to immune cells that release histamine, causing hives, itching, swelling, and bronchospasm – the sudden tightening of the airways - and, in some instances, anaphylaxis – a whole-body allergic response.
A subsequent study determined that the “allergen” was alpha-gal, a sugar molecule found in a portion of the monoclonal antibody and on the surfaces of cells in most mammals, except humans and other primates.
But why North Carolina and Tennessee? If the monoclonal antibody were the sole cause, severe reactions should have been more evenly distributed across the country. A key finding was that patients with new allergic reactions to red meat also had an IgE-specific antibody to alpha-gal. The cases were concentrated in the same southeastern pockets where alpha-gal sensitization was already unusually common. That pattern suggested that the drug was not creating the allergy so much as revealing one already present.
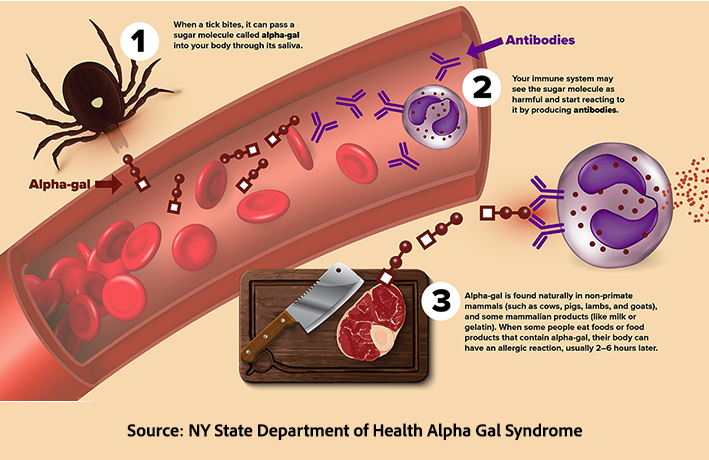
The missing link was a tick bite. In those regions, bites from the Lone Star tick, which carries alpha-gal, prime the immune system to produce IgE antibodies. Patients arrived for treatment already sensitized, turning a cancer therapy into a severe hypersensitivity reaction.
Why Diagnosis Is So Difficult
Alpha-gal syndrome (AGS) is a serious and potentially lifelong condition that results in allergic reactions to foods containing alpha-gal, including beef, lamb, pork, venison, rabbit, as well as cow’s milk and other dairy products. While rash and hives, signs of an urticarial reaction, along with GI upset, are the most common, there is an uncertain risk of anaphylaxis, which can be life-threatening.
The diagnosis of AGS is made difficult because symptoms most frequently develop several months after the tick bite and several hours after exposure to alpha-gal in a meal. The diagnosis rests on a suspicious history and evidence of alpha-gal sensitization, indicated by elevated IgE levels. Unfortunately, no firm IgE cut-off has been established, and higher titers do not accurately predict symptom severity. In the face of elevated IgE, physicians will recommend an alpha-gal avoidance diet for several weeks. If symptoms are not relieved, other allergic sources are considered. If symptoms do abate, continuation of alpha-gal avoidance is recommended. Despite all these caveats, it remains a diagnostic and treatment “crapshoot.”
Given the diagnostic and treatment difficulties, the best course of action is prevention, which includes removing any ticks you may encounter during your time communing with nature. And unlike it’s Tick breathren, the Lone Star Tick can be found on manicured lawns, picnic areas and even paved pathways.
The Tick That Changed the Map
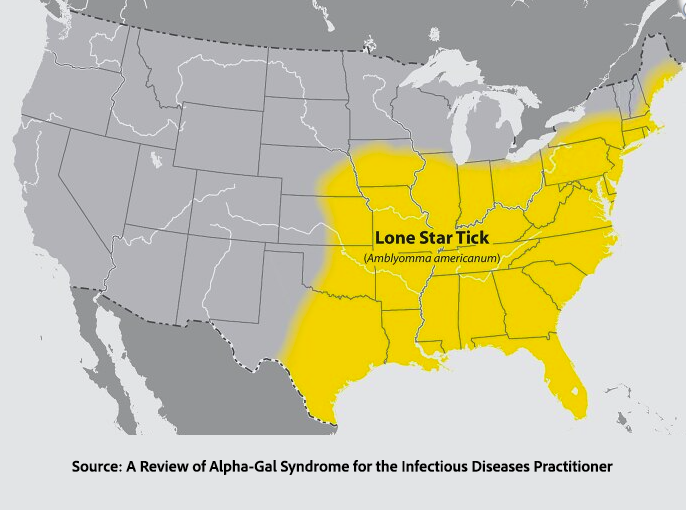 While several ticks have been associated with AGS, the primary driver is the “aggressive” Lone Star Tick, which is expanding its range in the US. Adults make their appearance from April to June and that prompted notification of all New York physicians by our Department of Health. The fortunes and habitat of the tick have followed that of its primary host, the white-tailed deer. In colonial times, the tick and deer were to be found across the Eastern seaboard. With the removal of forests, the tick and its host’s range diminished, but with conservation measures beginning in 1940, the Lone Star Tick is reclaiming its dominion. And the white-tailed deer also plays host to the tick associated with Lyme disease.
While several ticks have been associated with AGS, the primary driver is the “aggressive” Lone Star Tick, which is expanding its range in the US. Adults make their appearance from April to June and that prompted notification of all New York physicians by our Department of Health. The fortunes and habitat of the tick have followed that of its primary host, the white-tailed deer. In colonial times, the tick and deer were to be found across the Eastern seaboard. With the removal of forests, the tick and its host’s range diminished, but with conservation measures beginning in 1940, the Lone Star Tick is reclaiming its dominion. And the white-tailed deer also plays host to the tick associated with Lyme disease.
What was once an obscure regional syndrome is now a broader public health concern. On Long Island, where deer populations are robust and the Lone Star tick is increasingly common, alpha-gal syndrome is no longer rare enough to ignore.
According to the CDC, 4% of all AGS cases are in Suffolk County, Eastern Long Island. As the New York Times reports,
“The C.D.C. study suggests that between 3,800 and 18,000 people in Suffolk County had alpha-gal from 2010 to 2022. That corresponds to as much as 1.2 percent of the population.”
Yet awareness, surveillance, and reporting remain uneven. New York does not require systematic tracking of alpha-gal cases or of abnormal IgE test results, even as estimates suggest that thousands in Suffolk County alone may be affected. For clinicians, the condition remains easy to miss; for patients, it can be life-altering.
The lesson is less about a single tick than about a shifting landscape. As climate, wildlife, and human environments intersect, conditions once confined to specific regions are spreading into new territory. Alpha-gal syndrome is a reminder that disease boundaries are not fixed—and that a bite taken lightly today may carry consequences months later, at the dinner table.
Source: A Review of Alpha-Gal Syndrome for the Infectious Diseases Practitioner Open Forum Infectious Disease DOI: 10.1093/ofid/ofaf430

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


