
My Fall Into the Bone Health Debate
Back in February, in a rush to put some boxes in the basement, I tripped over a pile of misplaced carpet tiles and, “with the greatest of ease,” flew through the air before landing on my right arm and shoulder. As a physician, I have been called upon in several family emergencies to diagnose a broken bone in my sons or another family member. I am proud to say that my diagnostic skills have not suffered during my retirement, and that once again I misdiagnosed my humerus fracture as a strain, keeping my record of being wrong every single time intact. An hour later, at an urgent care center, the injury was more appropriately diagnosed, and I joined many in my cohort who had fallen and could or could not get up because of a fracture. A sling and six weeks solved my injury, but the memory sparked my interest in a recent study of the effect of calcium and Vitamin D on falls and fractures.
Calcium, Vitamin D, and the Dance of Building Bone
Bone seems so permanent, yet it is not inert scaffolding. The dance between osteoclasts absorbing old bone and osteoblasts laying down its replacement is too slow for us to notice, but over roughly ten years, we replace all of our bone. Two critical partners in the dance are calcium, the structural mineral substrate that fills the collagen matrix created by osteoblasts, and Vitamin D, the endocrine supply chain for calcium.
Calcium gives bones their strength and serves as a reserve for the body’s other uses of calcium, including nerve conduction. Low calcium makes our nerves more “irritable,” while too much leaves them weakened. As a result, our serum calcium levels are kept within a very tight range, and in the presence of a dietary deficiency, skeletal calcium is mobilized, weakening the bones.
Vitamin D promotes calcium absorption in the gut, helping to meet our daily needs. Vitamin D also affects our muscle function, and deficiencies are associated with weakness of the proximal muscles, i.e., those of the hips and thighs, more than the hands or feet. These muscles help us climb stairs, maintain a steady gait, and correct our balance when we stumble.
As we age, the dance between calcium and Vitamin D slows, even in the absence of nutritional deficiencies. Calcium remains within those strict limits, but there may be more turnover in remodeling and a gradual decrease in skeletal reserves, weakening the bone. Vitamin D, on the other hand, tends to decline more markedly due to less exposure of our skin to the sun and less conversion to its active form by the kidneys.
There is a disparity in bone loss between men and women. Beyond the background bone loss we all experience, women experience an “accelerated phase of bone loss” with menopause. A smaller subset of men undergoing treatment for prostate cancer with chemical castration will also experience a similar enhanced loss.
Aging Raises the Stakes
A fall is “an unintentional event that results in the person coming to rest on the ground or another lower level.” General estimates suggest that adults over the age of 65 are more prone to falls, with about a third experiencing at least one fall annually. Fractures are the most common serious injury resulting from those falls. As we age, an increasing fear of falling reduces our daily activity – the subsequent inactivity feeds back to make us increasingly frail, heightening the risk we seek to avoid.
Only about 5 to 6 percent of falls result in a fracture of any kind. But half of women and roughly 20% of men will sustain a low-trauma fracture during their lifetime, most frequently of the hip, wrist, humerus, and pelvis.
Why we fall remains poorly understood, but as with most aspects of aging, it involves a multiplicity of factors, including reduced vision, diminished strength and reflexes, and alterations in our gait and balance – all difficult to correct. While our loss of muscular strength may be apparent, the loss of bone mass that comes inevitably with aging is silent until it is not, and then presents as a fracture.
For falls, the risk of fracture depends on both the degree of trauma and the bone's resilience, that is, its strength. Age creates the perfect storm, with a rising incidence of falls and declining bone strength. Consequently, the incidence of age-related fractures rises dramatically as the amount of trauma required to cause a fracture declines. Prevention requires attention to preserving bone mass and reducing falls; however, once bone mass silently falls below a critical level, the only real treatment option is to prevent falls.
When it comes to Vitamin D and calcium, we can simplify this by noting that Vitamin D deficiencies increase both the frequency and severity of falls, whereas calcium deficiencies increase only their severity.
Early trials of Vitamin D and calcium supplementation reported significant reductions in fractures, with an absolute reduction of 2.5% for hip fractures and a relative reduction of 23%. However, the study population was enriched with older women, with a mean age of 84, low dietary intakes of calcium and Vitamin D, and all requiring residential care. These findings are not generalizable to a population without calcium or Vitamin D deficiencies who are living in the community, the broader population serving as the target market for calcium and Vitamin D supplements. A meta-analysis in the BMJ finds that the results differ markedly for this group.
What the Evidence Shows
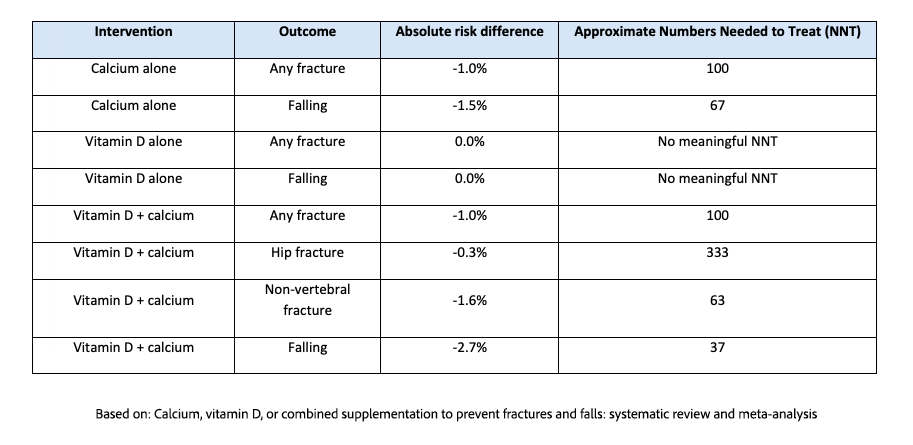
The researchers reviewed 69 studies involving more than 150,000 patients and considered the evidence to be of moderate to high certainty. For those who need to know right away:
“Based on absolute risk reductions and thresholds considered clinically meaningful, this review found little to no benefits from use of calcium, vitamin D, or combined supplementation on the prevention of fractures and falls.”
For those wanting a bit more, let’s start with the findings that neither calcium nor Vitamin D monotherapy had an impact on fractures, nor did combination therapy. Of course, there is the caveat that 3 studies showed an improvement of less than 1%, a value deemed below an acceptable clinical minimum.
We can also provide additional context using NNT, the number of patients needed to treat to reduce the incidence of fractures in 1 individual more than in the control group. For comparison, the NNT for statins to reduce myocardial infarctions is 77, and for nicotine replacement therapy to reduce smoking, it is 15. More germane are the bisphosphonates used to treat bone loss when medically indicated, where the NNT to prevent a fracture is roughly 10.
I would add that the confidence intervals for the absolute risk differences for calcium alone were too wide to reliably show a true benefit, and the remaining improvements were deemed clinically irrelevant, driven by one study of older, high-risk individuals in residential care.
When High-Risk Evidence Becomes Low-Risk Advice
A back-of-the-envelope estimate is that Americans without a clear medical indication spend roughly $1–3 billion annually on calcium and vitamin D supplements taken to promote “bone health,” although stricter estimates would cut those numbers by half. In any case, that is a lot of money for what is increasingly clear is little benefit.
Now, some may argue that taking Vitamin D has other benefits, that calcium loss is silent, that the cost is trivial, and that it has few adverse consequences. So why not? My answer, in keeping with the need for medical freedom, is, be my guest. [1] However, the greater issue is how a study of a high-risk population became the standard of care for those at low or no risk.
As the researchers point out, a systematic review of multiple medical guidelines found that 70% recommended Vitamin D supplements to prevent fractures or for general health. How did so many groups get it wrong? The easiest answer is that they generalized population-specific data to a population with a far lower risk. I am afraid that, by the nature of our research, this may not be a one-off case and helps explain why clinical trial results do not fully translate to real-world populations. To identify small but pertinent effects, researchers often choose populations with a higher incidence of a condition to generate a strong statistical association. We need not posit any ill intent; the only way to demonstrate a small effect is either with a very large population, which can be costly and time-consuming, or by enriching the population with more at-risk individuals.
The Real Lesson: Risk Matters
The real lesson is not that calcium and vitamin D are useless, nor that no one should take them. For people with documented deficiencies, poor dietary intake, osteoporosis, malabsorption, or other clear medical indications, supplementation has a role. But for the broad population of adults living at home who take these pills as insurance against fractures, the evidence increasingly shows the policy pays little.
Calcium and vitamin D supplements may seem benign, but decades of recommendations and billions of dollars later, “it can’t hurt” is not the same as “it helps.” The better question is not whether bones need calcium and vitamin D (they do), but whether more pills are the answer for people who are not deficient. The problem with guidelines is that studies of those at high risk are quietly exported to everyone else, turning targeted therapy into general advice and general advice into habit.
[1] The researcher pointed out that “it can’t hurt” does not apply to Vitamin D monotherapy, as their findings clearly demonstrated no benefit. More importantly, they note that calcium supplementation can cause mild but annoying GI effects, such as constipation, bloating, and abdominal pain.
Sources: Calcium, vitamin D, or combined supplementation to prevent fractures and falls: systematic review and meta-analysis BMJ DOI: 10.1136/bmj-2025-088050

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


