“Things were bad, it was terrible.”
- Lucas Henneman, lead author and professor at George Mason University.
Really? Air quality has indeed improved along with other more important factors like reduced smoking, but first, let’s scrutinize the Times reporting (as shown in quotes).
- The study published in Science has a paywall and is not accessible to the public.
- “Removing SO2 from flue gases was salubrious and a game changer for public health,” but SO2 per se has not been found to cause long-term health effects.
- Effects were analyzed by ZIP code, but since power plants have tall chimneys (~500 ft), their downwind emission patterns are not limited to the powerplant zip code.
- “Inhaling fine particles from coal was especially deadly,” but indoor air quality was not considered even though we are indoors 85% of the time.
- The analysis was based on a statistical index of fine particles emitted from coal combustion (Coal-PM2.5), which “dropped to 0.07 from micrograms per cubic meter in 2020 from 2.34 in 1999” but was not based on direct measurements.[1]
The Underlying study
The study underlying the Times reporting attempted to predict mortality responses to reduced coal emissions based on 2020 geographic patterns relative to 1999, which requires comparing patterns of potential confounders as well. A valid long-term mortality model could be expressed as functions of air pollution, smoking, economic status, age, race, diet, education, and lifestyle. All of these parameters vary among zip codes, but it is safe to assume that race, diet, education, and lifestyle remained essentially constant during adulthood.
Comparing temporal changes in mortality with changes in air pollution, smoking, and economic status avoids the need for geographic data on race, diet, education, and lifestyle factors that the researchers chose to ignore. But, this data is often difficult to obtain. A difference-in-difference analysis does not require this data, and I used measured PM2.5 to illustrate the concepts involving fine particle air pollution.
A quick aside: The difference-in-differences (DiD) method is a statistical approach used in observational studies to estimate the causal impact of a treatment or intervention. It involves comparing outcome changes over time between a treatment group, i.e., scrubbers, retirements, fuel changes, and a control group. The difference in the average change in outcomes for the treatment group compared to the control group before and after the treatment, the difference-in-difference helps control for time-invariant factors (race, diet, education, and lifestyle) and provides a more robust estimate of causal effects.
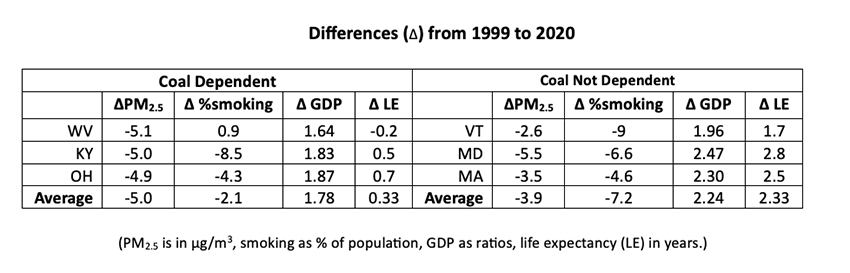
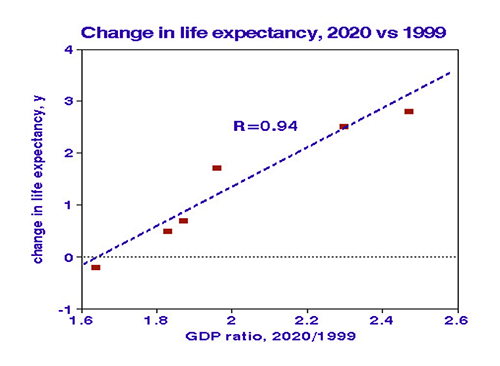 I compared changes in ambient air quality (PM2.5), smoking rates, and economic growth (GDP) in 3 coal-dependent states (KY, OH, WV) with those in three states not dependent on coal (MA, MD, VT). I used life expectancy at birth as the outcome measure since it accounts for differences in age distributions. In 2020, the “coal states” had half as much smoking, 28% less air pollution, 26% more economic growth, and two years longer life expectancy relative to 1999. [2] The strongest relationship with change in life expectancy was change in GDP, with a near-perfect correlation. Change in smoking was positively correlated with changes in PM2.5, but a statistical relationships between life expectancy and smoking or PM2.5 were not significant. Adverse effects of smoking are well established, as are benefits of economic well-being; long-term mortality benefits of reduced ambient PM2.5 remain to be confirmed.
I compared changes in ambient air quality (PM2.5), smoking rates, and economic growth (GDP) in 3 coal-dependent states (KY, OH, WV) with those in three states not dependent on coal (MA, MD, VT). I used life expectancy at birth as the outcome measure since it accounts for differences in age distributions. In 2020, the “coal states” had half as much smoking, 28% less air pollution, 26% more economic growth, and two years longer life expectancy relative to 1999. [2] The strongest relationship with change in life expectancy was change in GDP, with a near-perfect correlation. Change in smoking was positively correlated with changes in PM2.5, but a statistical relationships between life expectancy and smoking or PM2.5 were not significant. Adverse effects of smoking are well established, as are benefits of economic well-being; long-term mortality benefits of reduced ambient PM2.5 remain to be confirmed.
Timing.
Air pollution health effects depend on exposure patterns and duration and are classified as acute (over 1-7 days) or chronic (accumulated over decades). These two modes' relevant mechanisms, pollutants, and susceptible subjects differ substantially. Short-term (daily) deaths are limited to the frail elderly and have been associated with peak concentrations of various pollutants, including particulate matter and ozone, with a relative excess mortality risk of about 6%. Since they tend to operate smoothly over time, power plant emissions are not likely to be associated with peak mortality events like heat waves or stagnation episodes.
Long-term mortality relationships can be problematic. For example, accumulation over decades is required for smoking effects on mortality to be manifested with total exposures expressed cigarette pack-years. Based upon the accumulations over the study interval 1999 to 2020, 50 μg/m3-years, and the dramatic reduction, about 2.0 μg/m3-years, if coal-PM2.5 were a hazard during previous decades, those risks are long gone.
What Does It All Mean?
The study, taken at face value, demonstrates that coal-fired power plants would have contributed to pollution-related excess mortality in the past but not in the future. The New York Times statement that “coal is more harmful to human health” should have read “… was more harmful…”.
Moreover, since more important concurrent trends like smoking cessation or economics were not considered, those findings are meaningless. My simple example of a straightforward difference-in-difference analysis attributes the 1999-2020 mortality benefit to economics rather than air quality.
On a personal note, after studying this issue for ~50 years, I am dismayed that two of the nation’s premier publications have lent their names to such shoddy research.
[1] The sulfate portion of PM2.5, ostensibly water-soluble ammonium sulfate, has never been considered toxic. A current measure of sulfate was 3.4 micrograms per cubic meter.
[2]