
“Behavioral interventions such as mask-wearing, quarantine, restrictions on gatherings, physical distancing have been used to interrupt transmission of COVID-19 and to reduce the impacts of the pandemic.” Silubonde-Moyanda et al., Preventive Medicine, 2023.
By and large, such interventions have been didactic with little validation in the real world. Here, we use statistical analysis of survey data from the COVID States Project to evaluate their actual world performance.
The Survey
This online survey of individual COVID-related attitudes and behavior was conducted between April 2020 and May 2023 using state-level representative data for race/ethnicity, age, and gender reweighted to match the US population concerning race/ethnicity, age, gender, education, and residing in urban, suburban, or rural areas. The survey asked questions about exposure-related venues and protective behaviors. The polling frequency decreased over time, making more detail available during the pandemic's early and more severe phases.
Results
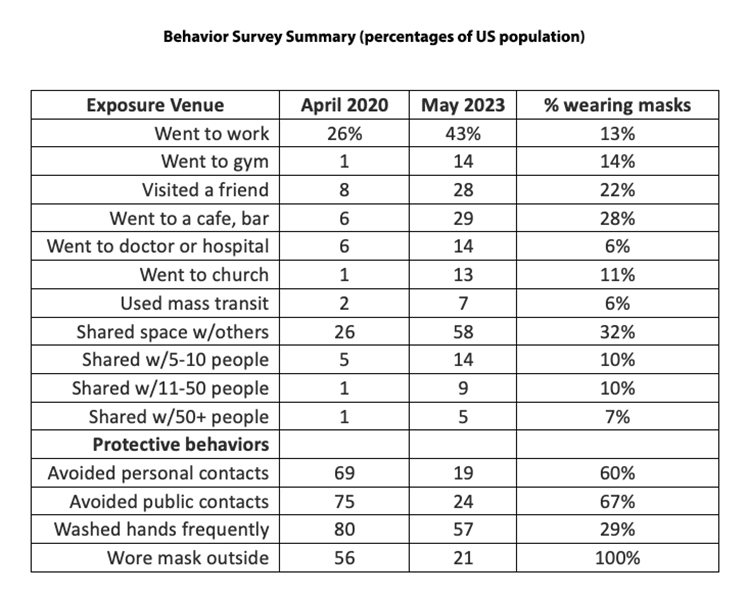
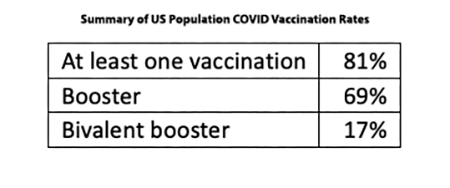
“Work” was the most common of the venues visited, which we interpreted as involving exposures[1] outside the home. “Gym” and “church” were the least visited. All exposure measures increased over time as concerns about virus transmission relaxed; the most common exposure involved work and shared spaces. As with other behaviors, participation in various actions varied across the country – we remain geographically and behaviorally diverse—for example, the District of Columbia the most highly vaccinated and Wyoming the least.
Protective behaviors decreased substantially during the pandemic, more than 3-fold for contact with others but less for regular mask use. “Frequent handwashing” was an exception, but those responses depend on the definition of frequent.
We suspected many of these statistics were intercorrelated in that those who visited these venues were less likely to be masked, leading to the negative relationships between masking and exposure shown in the right-hand column. For example, only 13% of mask wearers went to work, and only 6% used mass transit. This interdependence must be considered when evaluating the effectiveness of a protection measure. It seems likely that mask wearers will also adopt other highly correlated measures, precluding assigning benefits to any of them.
Trends
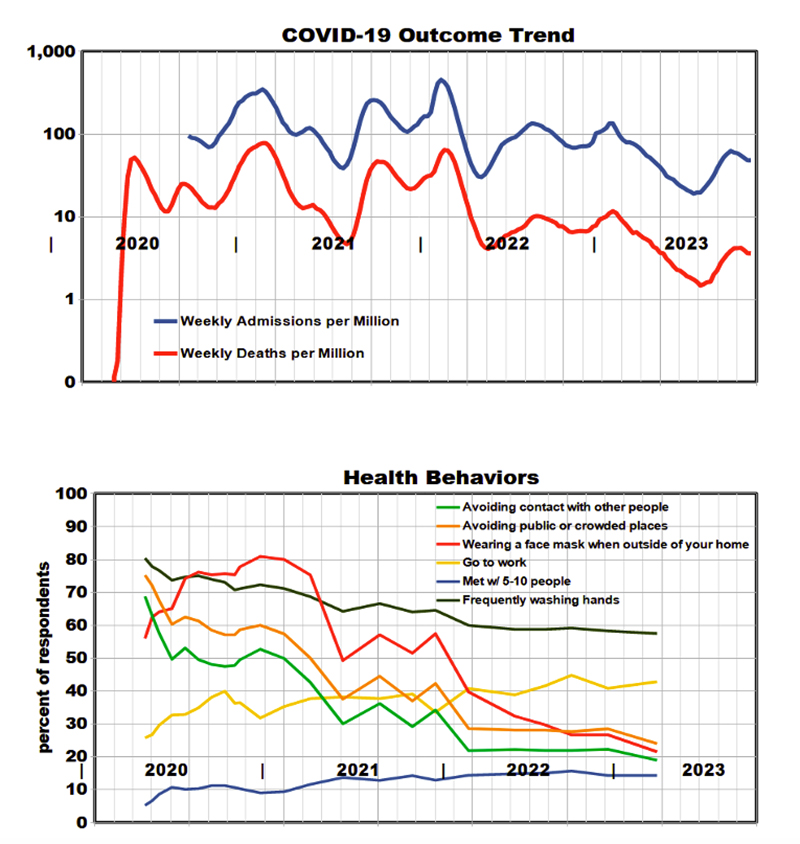
The graphs provide details on national trends during the pandemic with hospital admission and death rate outcomes and selected behavior parameters to represent exposures.
- Outcomes show peaks and valleys as virus variants emerged and vaccines became available.
- Admission rates held relatively steady through 2022 and then began to decline.
- Death rates declined consistently, beginning in 2021.
- Potential exposures increased, protective activities decreased over time, but outcomes improved.
- We found state-level trends similar to national trends.
Dose-Response Relationships
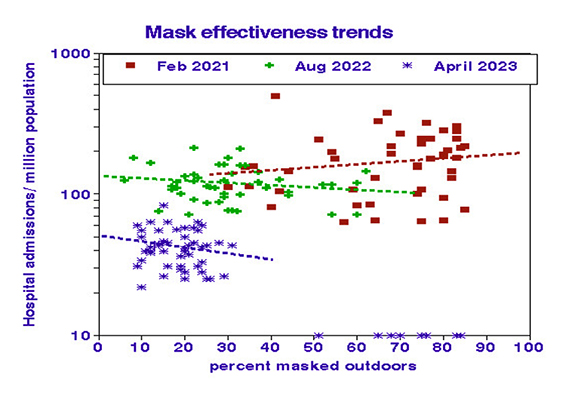 The ultimate use of such behavioral data is to evaluate relationships with outcomes. The disparate trend lines shown above suggest that relationships changed during the pandemic. Using state-level data, we partitioned the pandemic into three consecutive periods, assessing hospital admissions against masking frequency for each period. The beneficial effects of masking on admission rate improved over time, suggesting that other factors prevailed during the early stages of the pandemic. Without stratification by time, the overall dose-response relationship would demonstrate increased masking, leading to more admissions. This counterintuitive observation results from the overall reductions in masking and admissions, with hospitalizations decreasing faster (~10-fold) than masking (~3-fold), suggesting that masking may have remained effective as the pandemic waned.
The ultimate use of such behavioral data is to evaluate relationships with outcomes. The disparate trend lines shown above suggest that relationships changed during the pandemic. Using state-level data, we partitioned the pandemic into three consecutive periods, assessing hospital admissions against masking frequency for each period. The beneficial effects of masking on admission rate improved over time, suggesting that other factors prevailed during the early stages of the pandemic. Without stratification by time, the overall dose-response relationship would demonstrate increased masking, leading to more admissions. This counterintuitive observation results from the overall reductions in masking and admissions, with hospitalizations decreasing faster (~10-fold) than masking (~3-fold), suggesting that masking may have remained effective as the pandemic waned.
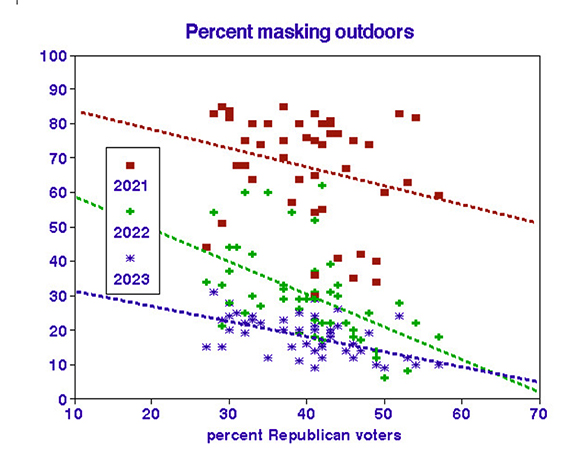 We did find strong relationships between masking and voter registration. As the severity of COVID outcomes declined, protective measures followed suit, with similar demographic relationships.
We did find strong relationships between masking and voter registration. As the severity of COVID outcomes declined, protective measures followed suit, with similar demographic relationships.
Conclusions
No single exposure or protection measure prevailed during the pandemic, thus shedding doubt on our previous analyses that considered such measures singly. Protection by mask or vaccine has been evaluated in the laboratory, whereas this evaluation is based on our behavior. The apparent benefits of masking, as determined in the field, include additional benefits from associated handwashing and social separation.
With credit to ChatGPT and apologies to E.A. Poe:
In shadows cast by unseen foe,
A pandemic’s dirge began to grow.
A silent specter, cold and sly,
Crept through the world with a mournful sigh.
Masks adorned, a somber dance,
A shield, perhaps by chance.
Vaccines rose, a beacon light,
A remedy to end the night.
In vials held, a potion bold,
These tales of science to be told.
Limitations
This observational study suffers from the usual distinctions between individual and population behaviors. It was restricted to internet users and thus may have inadvertently been biased.
[1] Many of the survey questions asked about travel to various locations outside the home that we designate as changes in “exposures” since they may involve differences in ambient COVID aerosol.


