
Despite advances in radiation and chemotherapy, surgery, and often time complex surgery remains an important tool for treating cancer. Surgery is considered more of performance art, which by the way is true only in degree as compared to the prescriptive arts of chemotherapy or radiation, and is often performed more safely in centers with greater experience due to larger volumes. Does a flagship hospital if among the best, provide a halo of goodness and safety to its network affiliates? While the branding may say yes, the data says no, or at least “let the patient beware.”
The retrospective study is reported in JAMA Network and involves Medicare data on the approximately 30,000 patients undergoing cancer surgery between 2013 and 2016 with a simple endpoint, were they dead or alive 90 days after surgery. The flagship hospitals were those rated among the top 50 by US News and World Report at least once during the same period. Before proceeding, that data is itself engaging in that over those three years, only 59 hospitals were named to the top fifty – there is very little change over time, much as we see in other varied fields, like top businesses or sports franchises. Additionally, as a sense of how healthcare continues to consolidate, 90% of these top hospitals had affiliates, and by that, I mean hospitals that incorporated the flagship hospital’s name with their own – a clear attempt at branding.
Overall the study looked at 59 hospitals, with 343 affiliates, with roughly 17,000 patients undergoing complex cancer surgery at the flagships and 12,000 patients treated at the affiliates. While patients were a bit older at the affiliates, the comorbidities were similar so to that extent we seem to be comparing apples to apples. In addition to 90-day mortality, the authors calculated a standardized mortality ratio, SMR, which calculates the expected mortality using a range of variables and compares it to the actual morbidity – smaller numbers reflect greater “safety.”
- The 90-day mortality was higher at the affiliated hospitals, as a group than at the flagships. This was true for all five procedures [2] aggregated and for them individually except for esophagectomy – removing the esophagus, the tube connecting the mouth to the stomach, a particularly difficult operation in all hands.
- SMRs, the measure of safety, was better than the national average for 80% of the top-ranked hospitals and 34% of the affiliates, again all the hospitals were aggregated.
- The flagships outperformed their affiliates 84% of the time.
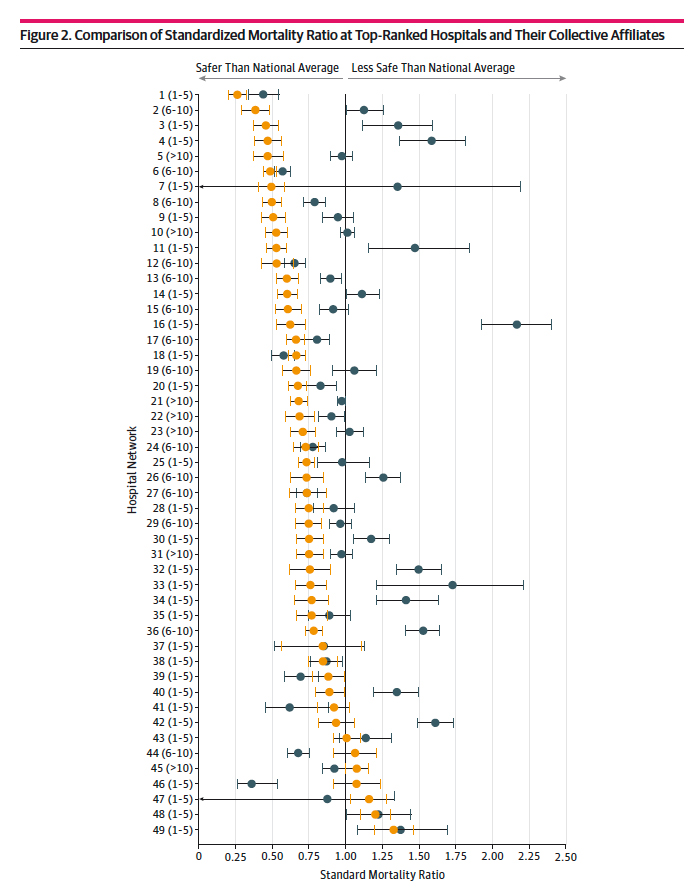
Orange circles are the flagships; the blue circles show the range of SMRs for their affiliates.
It is difficult for patients to know where the best care might be found. Prior studies show that while tools for comparing hospitals are available, they are used infrequently. Patients rely on the recommendation of their physicians, to a larger and larger degree, employed captives of hospital networks or family and friends. As healthcare is further changed from bespoke personalized care to a commodity, hospitals have made greater use of the tools of commerce, in this case, branding. And it does make a difference. A survey of American adults showed that while 85% would travel an hour to a hospital for complex surgical care, a third of them would remain in their community if a flagship hospital network affiliate was in the community; and roughly half of those individuals thought that the affiliates were comparable to the flagships.
Brand recognition works because brands offer a consistent product; the meals don’t change from one Cheesecake Factory to another. I know that surgery can be more complicated than a Bang-Bang Chicken and Shrimp, but if hospital networks are serious about branding their name and care these differences between the hospitals in their system need to be addressed and fixed. They could require more complex cases to be sent to the flagship, but that would clinically enrich the hub while impoverishing the spokes and over time require patients to travel for treatment. Or they might find ways to enhance the care in the spokes, but that requires a more significant effort than an affiliation agreement and some shared oversight. In either instance, I agree with the authors, “hospitals must assume some responsibility for leveraging relationships with their affiliated hospitals to ensure that the safety and quality of care is optimized at all hospitals that adopt their trusted brand.”
[1] Observed Deaths/Expected Deaths e.g., we expected 5 patients to die, only three did, so the SMR is 3/5 or .6; alternatively, we expected 5 patients to die and 8 did, so the SMR is 8/5 or 1.6. Hospitals with small volumes may appear worse or better simply because of 1-off events in a small sample.
[2] Removal of a portion of the lung, lobectomy; removal of the large intestine, colectomy; removal of the stomach, gastrectomy; removal of the esophagus, esophagectomy; and removal of the pancreas and duodenum, the trick here is to put everything back together, pancreaticoduodenectomy.
Source: Differential Safety Between Top Ranked Cancer Hospitals and Their Affiliates for Complex Cancer Surgery JAMA Open Network DOI: 1001/jamanetworkopen.2019.1912

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.



{kind=link}