It is a given, at least in healthcare involving procedures, that more experience results in better outcomes. The “more experience” requires both the judgment of which patients are best suited for a procedure as well as some of the nuanced hand-feel that cannot be taught only recognized and learned. Often we speak of a steep learning curve, which by the way is a misnomer, as rapid movement up suggests faster learning; the problematic curves are the flat ones with little change over time. A paper in Circulation Cardiovascular Interventions opens the window on that period before experience, when physicians are learning.
A bit of background
The increasing speed of technologic change means that much of what a physician learns does not take place in the protected environment of a training program. In many cases, skills are transferable from residency or fellowship, but again, judgment and hand-feel not so much. During my surgical education in minimally invasive care, that came along ten years or more later and I had to learn in real-time, with my patients, and without necessarily the safety net of an older, wiser mentor. This is the setting for this study, involving cardiologists who are now attempting to minimally invasively open completely occluded coronary arteries, what was once the purview of cardiac surgeons who bypassed the blockage.
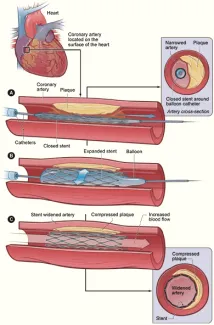
The first, and perhaps the greatest challenge in getting across a completely occluded artery is to get a wire across the blockage, a wire that will provide the “rail” for the rest of the procedure. It is difficult to push a wire that is perhaps three times the thickness of the period at the end of this sentence, through a blockage 3 feet away. You may not get across, you can perforate the artery itself, and even after crossing the lesion, you may not be able to successfully dilate and stent the vessel.
The Study
The American College of Cardiology maintains a national database of all cardiac catheterizations, their indications, complications, and outcomes, and serves as the source of information. Over a six-year interval, they identified 2% of the 4.2 million total catheterizations, that involved these total occlusions; procedures in 1500 hospitals involving 7500 interventional cardiologists. The newbies, 72% of the cardiologists involved, were defined as having done less than 10 of these procedures in their first year, the early adopters, those having done more than 20, represented 14% of the group.
For the entire registry, 73% of the time the blockage was successfully crossed with a wire, and of those patients, 80% were successfully opened for a total success rate for “all-comers,” of roughly 60%. 4.2% of patients experience a major adverse cardiovascular event. Significant bleeding was the most common complication at 4%, 1.4% of patients experienced perforation of their artery, 2% had a myocardial infarction. The results are captured in these charts:
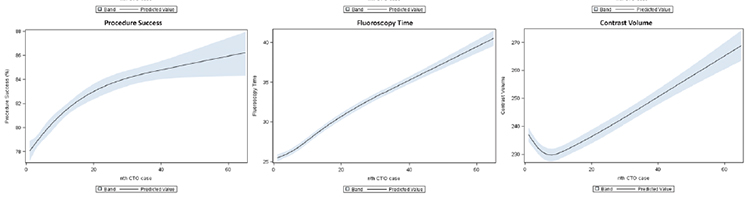
As you would expect, procedural success increased with case volume (the horizontal axis). The increase in fluoroscopy time, a measure of the length of the procedure, and volume of contrast used, a rough measure of difficulty, also increased with experience. As the operators became more experienced, they were less tentative, more persistent. As to complications:
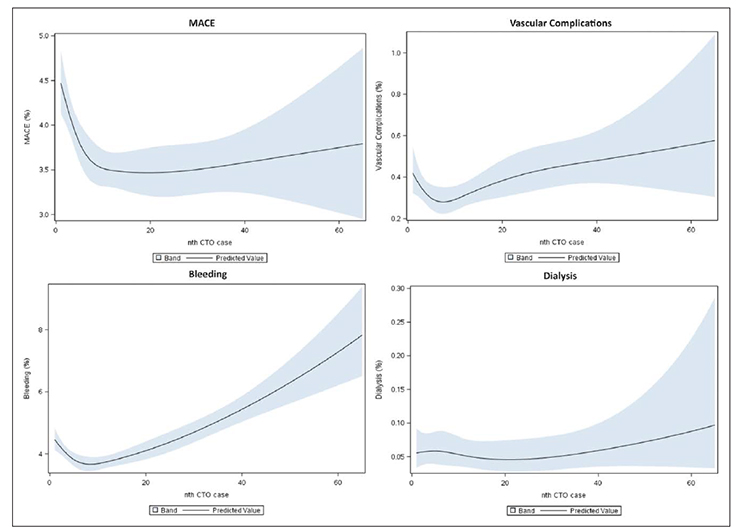
It took roughly the first ten cases to bring those major adverse consequences down and then they remained relatively constant. The increase in bleeding most likely reflect those longer and longer cases, that perseverance that requires a longer period of anticoagulation and manipulation. Vascular complications and the need for dialysis, often a result of that increased use of contrast, also follow from that “need to succeed.”
There was little difference in the learning curves of the newbies versus the more enthusiastic early adopters. The early adopters, as you might anticipate, took on more elective patients with greater co-morbidities; the newbies were a bit more tentative attempting these procedures when revascularization was more emergent.
The researchers did provide us with some real-world data on the learning curve. It isn’t pretty initially but quickly settles (regresses?) towards the national averages. Experience expands the population that is considered treatment candidates and results in increased complications.
At least two questions remain unanswered. Those light blue regions in the graphs show the confidence interval for those trends; they are pretty wide as time goes on – does that mean that some physicians are just better at one procedure over another and that there is a limit to how much experience improves your outcomes? After all, bad technique, evenly constantly practiced, does not lead to better results. Second, how much of that learning curve could be avoided if these practitioners were being mentored by more experienced physicians rather than being the pioneers? It would be interesting to see and compare the learning curve of fellows under direct supervision with these results.
Source: Examining the Operator Learning Curve for Percutaneous Coronary Intervention of Chronic Total Occlusions Circulation Cardiovascular Interventions DOI: 10.1161/CIRCINTERVENTIONS.119.007877

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.



{kind=link}