
Post-marketing surveillance of Pfizer’s and Moderna’s COVID vaccination has identified a possible association between its use and subsequent episodes of myocarditis and pericarditis – two forms of heart inflammation. Pericarditis involves the inflammation of the sac containing the heart, which acts as a buffer of the heart’s beat and causes discomfort from all that motion when inflamed. Myocarditis is an inflammation of the middle layers of the heart’s wall, and it too causes pain and may lead to the heart failing its function in fully circulating our blood. Both pericarditis and myocarditis are associated with viral infection, although the underlying cause is unknown in many cases. Both are generally self-limiting problems that resolve with medical support instead of medical intervention.
The Study
The research is based on Ontario, Canada’s system for reporting adverse events after COVID immunization between December 2020 and September 2021. Reporting is mandatory for healthcare professionals and voluntary for patients or their caregivers. So we can say at the start that the total number of adverse events is undercounted, but probably not by an order of magnitude. Those cases where the patient shrugged off a twinge and didn't seek care, do not represent significant morbidity. There were roughly 19.7 million doses of the mRNA vaccines administered and 417 cases of myocarditis or pericarditis found in the Ontario registry.
The diagnosis of myocarditis or pericarditis can be uncertain; very few are lining up for a biopsy of their heart to provide histologic proof. The researchers categorized the uncertainty of the myocarditis and pericarditis cases using the Brighton criteria. The Brighton Collaborative, which was founded long before COVID in 2001, is an international effort to define the adverse effects of immunization. Their methodology has been adopted in many countries, including Canada. Brighton defined three levels of certainty associated with myocarditis and pericarditis: Level 1, a definite case, confirmed biopsy or MRI, Level 2, and Level 3, a possible case, based upon symptoms, an abnormal EKG, and some biomarkers of inflammation not of cardiac injury (e.g., c-reactive protein). Using these definitions, the researchers identified 71% of the reported cases as meeting one of the three levels of certainty. Of these 297 cases:
- 69.7% occurred after the second dose of the vaccine
- 76.8% occurred in males
- Median age 24
- Roughly a third of cases were pericarditis, a third myocarditis, or and a third both
- The median time to onset of symptoms was within three days of vaccination, with most cases identified within seven days.
- The incidence of myocarditis and pericarditis was higher after the second dose, more so with Moderna’s vaccine, and more frequently among males.
- The group with the highest case rate of 300/1,000,000 (0.03%) was males, 18-24 after the second dose of Moderna. An adverse response to Pfizer’s vaccine was lower: 59/cases per 1,000,000 shots (0.006%).
- The second highest group was males aged 12-17, with a case rate of 97/1,000,000 (0.01%)
- Essentially all of these patients were seen in the ED; 70% were admitted, and 5% to the ICU. There were no deaths [1]
More Data = Better Data
Much of this has been known since early in the mass vaccination programs but what follows comes from recognizing that percentages will change as the numerator, the number of cases, and the denominator, the number of vaccinated individuals change – that is just math. More importantly, having patience enough to wait for the longer term, more defined, “better” information can be helpful.
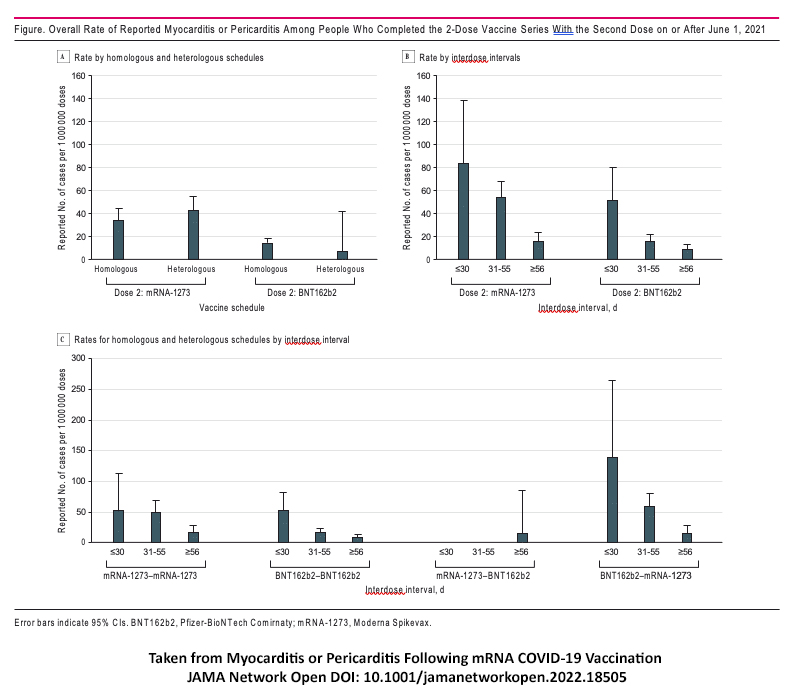
The incidence of myocarditis and pericarditis decreased as the interval between vaccine dosages increased. Mixing the doses given, one of Moderna and one of Pfizer, a heterologous schedule also resulted in a reduced case rate for these adverse effects.
These results are in line with those seen in the US. But here is where our friends to the North differed: Rather than stop vaccinations or whip up a politically driven angst, they chose to change their approach when the evidence changed. They began to preferentially offer the Pfizer vaccine to the more at-risk younger males and issued guidelines that recommended a longer interval between doses.
Comparing the Adverse Effects of the Vaccine With Covid Itself
Finally, to give all these numbers some context, consider a study done on patients hospitalized with COVID in the US during a similar period. [2]
- The incidence of myocarditis in hospitalized patients, if they did not have COVID (the control group), was 0.009% - just slightly more than the case rate in the highest vaccinated group who received a Pfizer vaccine and 3-fold less than those receiving a Moderna vaccine.
- The incidence of myocarditis in hospitalized patients with COVID for the same age groups was 24%
- This month, 18-29 year-olds represent 16% of all COVID cases.
Getting it Right
Understandably, amid an evolving pandemic, we will get things wrong. It is less understandable that we would attribute these errors to evil intent. I am not suggesting that we do not act on the information we have, but that we are a bit more humble in presenting and refuting those findings as the data evolve. As with any other drug or therapy, adverse effects will inevitably be present. But it is critical to consider the effects along with the benefit of the treatment. Failure to do so can only provide slanted and incorrect information to the public, just about the last we need during the pandemic. Last word to the researchers,
“Of importance, the risk of myocarditis or pericarditis following receipt of mRNA vaccines also needs to be considered in association with risks of myocarditis following SARS-CoV-2 infection (i.e., higher rates of myocarditis following infection than vaccination) and the high effectiveness of mRNA vaccine products. … These results will also be helpful in the ongoing contextualization of the risk of myocarditis or pericarditis following receipt of mRNA vaccines compared with the risk of SARS-CoV-2 infection and associated outcomes.”
[1] Remember that these patients sought and received medical attention and may reflect an overestimate of severity. The percentages have been rounded.
[2] Again patient selection of the hospitalized overestimates the impact of myocarditis, but it is a relatively apples-to-apples comparison since the same criteria were used in the Canadian study.
Source: Myocarditis or Pericarditis Following mRNA COVID-19 Vaccination JAMA Network Open DOI: 10.1001/jamanetworkopen.2022.18505

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.

