You just can't hype drugs. They are either going to work well or not. Wishful thinking doesn't help. Neither does bluster. Nonetheless, we're now getting quite a dose of hype and bluster in recent days. Chloroquine has been in the news as a result of its known anti-coronavirus activity, but perhaps even more so because it's getting a public buzz that it doesn't deserve. Let's take a look at what's really there.
I previously discussed the in vitro ("test tube") assays of the potency and selectivity of remdesivir and favipiravir, two of the many known drugs (both approved and experimental) that are being evaluated as potential coronavirus drugs. Let's do the same for chloroquine, which is big news, mostly for the wrong reasons.
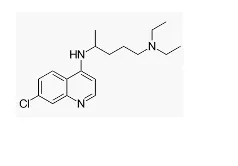
CHLOROQUINE
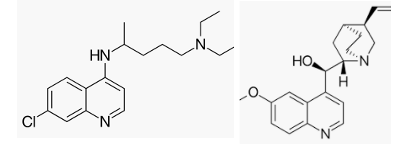
The chemical structures of two malaria drugs, chloroquine (Left) and quinine (Right)
WILL CHLOROQUINE STOP CORONAVIRUS REPLICATION?
Chloroquine, which was discovered in 1930s, was used extensively to treat malaria beginning the 1960s. By the 1970s multiple strains of malaria developed resistance to the drug and it became little-used. Chloroquine may be of little use against malaria but it could be an entirely different story for coronavirus.
As the frantic search for repurposed drugs to combat coronavirus continues, large numbers of drugs have been tested for anti-coronavirus activity. A number of "hits" (a drug or chemical compound that tests positive in the antiviral assay) have been discovered. One of these is chloroquine. Although it is not intuitively obvious why chloroquine should have antiviral properties (it was used to treat a completely different pathogen – parasite, as opposed to a virus) it does so anyhow (1). And it's fairly effective in inhibiting the replication of coronavirus in cells that are infected with the virus. Figure 1 shows the relative potency of chloroquine and four other known or potential antiviral drugs.
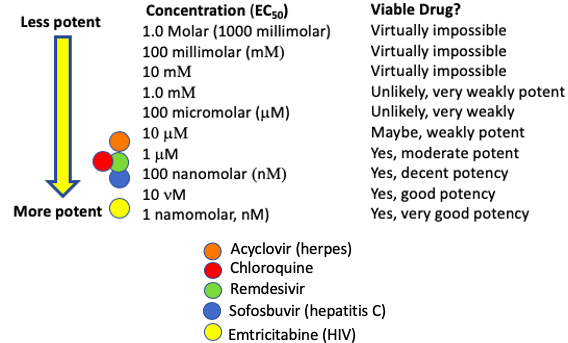
Figure 1, Five known or experimental antiviral drugs and their EC50 values in cultured cells.
The anti-coronavirus properties of chloroquine and six other experimental drugs were published in a recent letter published in the journal Nature. Chloroquine does a good job inhibiting viral replication in cells.
I've already written similar articles about remdesivir and favipiravir. Chloroquine, when compared to the others in Figure 2, looks pretty good.
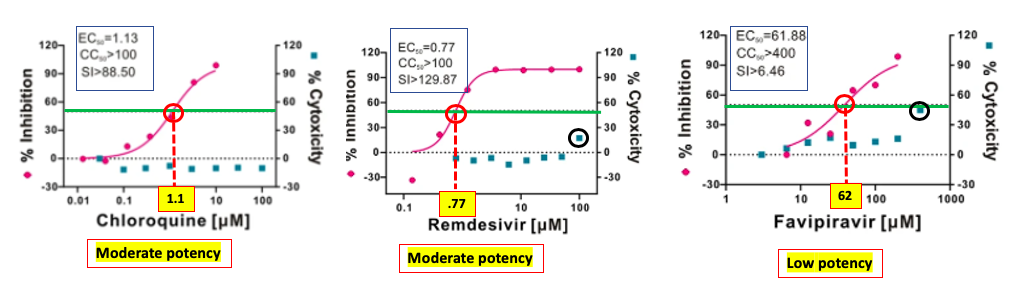
Figure 2. The potency and cytotoxicity of three potential coronavirus drugs. The lower the EC50 the more potent the drug.
In Figure 2 chloroquine (left) inhibits 50% of the growth of coronavirus in vitro at a concentration of 1.13 micromolar (this is the EC50 (1) - where the pink curve meets the red hatch line). The blue squares represent cellular toxicity; chloroquine shows absolutely no sign of cellular toxicity at concentrations up to 100 micromolar, giving it a selectivity index (SI) of at least 88.5 and probably much higher. To put this data in perspective, a drug with an EC50 of 1.13 micromolar is not spectacularly potent, but is good enough to lie within the range of other antiviral drugs. The profile of remdesivir (Center) is similar to that of chloroquine; it is moderately potent (EC50 = 0.77 micromolar) in stopping viral replication and also has negligible cytotoxicity. On the right is Favipiravir is a very weak inhibitor of viral replication (EC50 = 62 micromolar), which begins to show signs of cellular toxicity at a concentration of 400 micromolar. Source: Nature.
TOXICITY
Right away we run into an apparent contradiction. Chloroquine appears to be non-toxic to the cells in the assay but in real life, the drug can be quite toxic. How toxic? It depends on who's running the experiment. Estimated lethal doses in humans (assuming an average weight of 70 kg/154 pounds) can be obtained from the PubChem database. Suffice it to say that the results aren't especially consistent.
- Journal of Forensic Science - 21 g
- Japenese Journal of Toxicology - 9.6 g
- Postgrad Medicine J - 42 g
- Human Toxicology - 0.6 g (600 mg)
- Journal of Clinical Toxicology - 1.7 g
- Archiv fuer Toxikologie - 12.5 g
- Wuhan Institute of Virology - 2-4 g
Obviously these numbers are all over the place. We can immediately throw out the number from the journal Human Toxicology, since the lethal dose they report (600 mg) is the same as the average daily dose for malaria. If we also treat the 42-gram data as an outlier it is fairly safe to conclude that a single lethal dose of chloroquine in humans is in the 2-20 gram range, meaning that it has significant toxicity. Common side effects include:
- blurred vision
- nausea
- vomiting
- abdominal or stomach cramps
- headache
- diarrhea
- temporary hair loss
- changes in hair color
- muscle weakness
Furthermore, the use of the drug can result in severe retinal damage which can be permanent. Chloroquine suicides have been documented in the literature. And recently, there have been poisonings of Nigerians who mobbed pharmacies in order to take the drug prophylactically after President Trump spoke about it (3).
WHY THE DISCREPANCY?
You may be wondering why chloroquine, which appears to be non-toxic in cell-based assays, is a rather toxic drug. The answer is simple. The cells used in the tests are called Vero E6 cells. These cells, which were originally isolated from the kidneys of African green monkeys, can be easily grown in culture media and are widely used for in vitro studies (2). (The science of cell cultures is beyond the scope of this article.)
But humans are not made up of Vero E6 cells, so the absence of toxicity in a single cell line does not mean that the drug won't have organ or systemic toxicity in animals or humans. This kind of information is usually picked up in Phase I (safety) clinical trials. Unexpected toxicity is far less likely to occur when dealing with approved drugs; its toxicity profile from prior Phase I trials has already been established.
CLINICAL TRIAL DATA (SUCH AS IT IS)
Unlike remdesivir, which is now being evaluated in hundreds of clinical trials, chloroquine isn't attracting as much of an audience (4) as others, such as remdesivir. The only human "data" of efficacy I can find is the English translation of the abstract of a Chinese paper. It is hardly convincing.
"Here we found that treating the patients diagnosed as novel coronavirus pneumonia with chloroquine might improve the success rate of treatment, shorten hospital stay and improve patient outcome."
"[A group of experts a consensus] after extensive discussion. It recommended chloroquine phosphate tablet, 500 mg twice per day for 10 days for patients diagnosed as mild, moderate and severe cases of novel coronavirus pneumonia and without contraindications to chloroquine."
PREDICTION: WILL CHLOROQUINE BE A GAME-CHANGING CORONAVIRUS DRUG?
Unlikely.
LESSONS (THAT SHOULD BE) LEARNED
Two people, both with very large audiences, made incorrect statements about the drug. There could not be a worse time for this. President Trump has one of the preeminent scientists in the world, Dr. Anthony Fauci, as the de facto leader of the White House Coronavirus Task Force, yet the president occasionally dispenses advice that contradicts Fauci. This is like teaching Steph Curry how to shoot a basketball. This needs to stop. Incorrect information at this time can be deadly.
And then there's Elon Musk...
Elon Musk - please shut up. You don't know what you're talking about. I would suggest a trip to Mars in one of your spaceships. One way.
Next: Hydroxychloroquine – Chloroquine's Safer "Cousin."
NOTES:
(1) Chloroquine is said to work by inhibiting the entry of coronavirus into cells in the lung, a key step in viral replication. This is not the first drug to work in this manner. There are several HIV/AIDS drugs that work just this way.
(2) In vitro literally means "out of the body." It refers to experiments performed with cells, not living animals, etc.
(3) The president stated that chloroquine is FDA-approved for the treatment of coronavirus infection. This is incorrect. But since it is approved for malaria it can be used off-label for other purposes.
(4) Chloroquine is one of the drugs being evaluated in the WHO SOLIDARITY trial.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


