
Diabetes is a disorder of glucose metabolism. For a variety of reasons, your glucose levels are too high, and your body contends with this excess by, among other changes, increasing plaque in arteries which results in higher rates of cardiovascular disease. If we could only nip the process in the bud, so to speak, we might avoid a lot of death and destruction and reduce health care costs.
Pre-diabetes is a constellation of metabolic measures that prior research has shown to proceed the onset of diabetes. As with most science, there is a disagreement about which of those measures, those biomarkers, are most important. The researchers looked at the criteria supported by the American Diabetes Association, the International Expert Committee (IEC), a global consortium of endocrinologists, and the WHO. [1]
The study population was taken from the Atherosclerosis Risk in Communities (ARIC) study, which began in 1989. More specifically, they took individuals age 71 or greater who were seen on their fifth survey visit, roughly 24 years into the study. There were 3400 participants without diabetes, 60% female and 17% black, median age 75.6.
The prevalence of pre-diabetes varied with the definition. 73% met the ADA definition, 15% the IEC definition, and 23% the WHO definition. They were follow-up at a visit five years later. 2500 made those visits, 434 of the original cohort had died. One hundred fifty-eight had a diagnosis of diabetes during that interval.
- Pre-diabetes was associated with the onset of diabetes. The increased varied with the criteria used to define pre-diabetes but ranged from 3 to 8-fold. The broader the criteria, i.e., the ADA definition, the more cases of patients going on to diabetes identified.
- Pre-diabetes was not associated with mortality.
You might be right in concluding that pre-diabetes was a useful construct to identify a risk of diabetes but not a risk of dying. Depending upon how useful you thought this pre-identification was in preventing diabetes, you could shutter or widen the diagnostic gates using the ADA, IEC, or WHO criteria. But you would be missing some important information. What happened to the rest of those pre and non-pre-diabetic individuals? Here is the telltale graph.
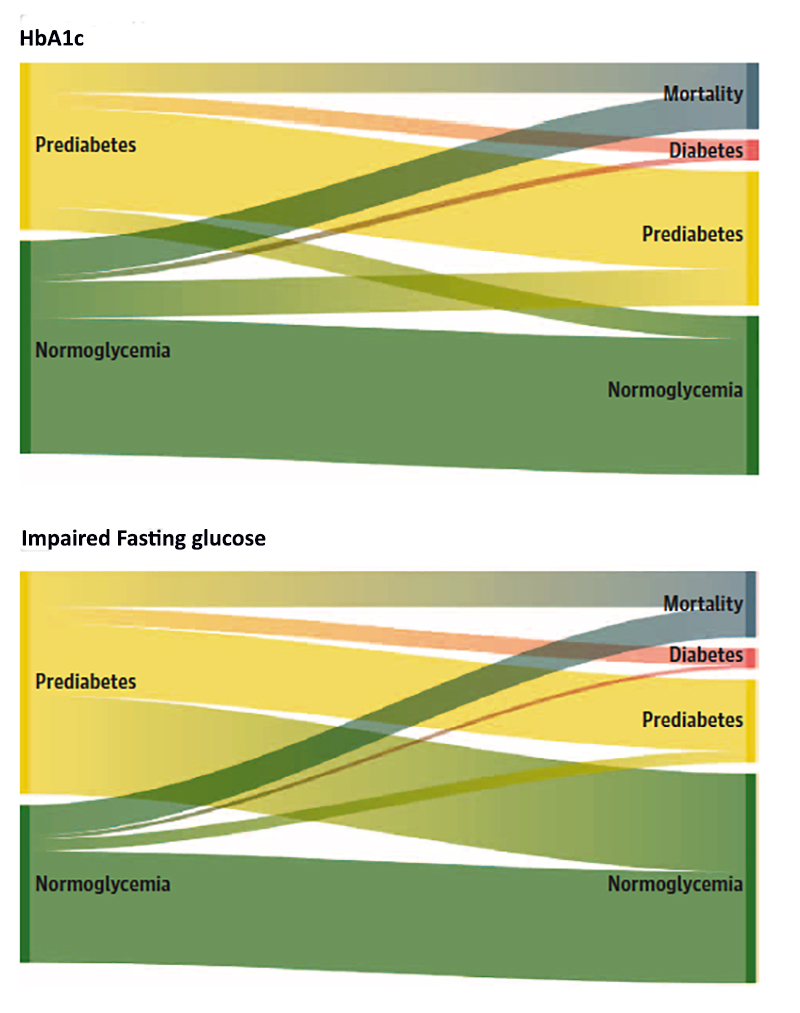
It shows the status changes for patients determined to be pre-diabetic based upon their HbA1c or impaired fasting glucose over time.
Fewer than 12% of individuals went from pre-diabetes to diabetes during this nearly six-year interval, no matter how the diagnosis of pre-diabetes was defined
13% of those with an elevated HbA1c returned to normal, 44% of those with impaired fasting glucose returned to normal. More individuals were normal than abnormal based on a diagnosis of pre-diabetes.
In this older age group, pre-diabetes does not seem to have any relevant predictive value.
“Given the low risk of diabetes progression in this study (especially relative to mortality risk), it is unlikely that pharmacologic intervention or other aggressive approaches to diabetes prevention in older age will provide large benefits and could have unintended harmful effects…”
Patients with pre-diabetes are counseled to change their lifestyle, better diet, more exercise. Both reasonable and benign suggestions. Both suggestions could be offered without screening for diabetes, let alone labeling patients with this “pre” condition.
An important caveat
Diabetes is increasingly harmful over one’s lifetime. A handy rule of thumb is that for every year one is diagnosed with diabetes, it adds an additional year to your chronologic life – 5 years of diabetes in an individual age 70 makes them 75 physiologically. So this study should be repeated for a younger age group, late 50 to ’60s. Perhaps the transitions are different and would warrant more aggressive surveillance.
The editorial accompanying the research makes an important point. The ravages of diabetes upon your health develop over time, so in a sense, diabetes is a risk factor for “accelerated dying.” Pre-diabetes is a risk factor for diabetes and is “twice-removed” from the outcome to be avoided, dying sooner rather than later. I admit that this is a bit of sophistry, but it contains a truth. Those ADA criteria that categorized 73% of people as pre-diabetic did more to create concern than improve results – especially when you realize that pre-diabetes diagnosis results in even more surveillance and the anxiety involved in awaiting results, let alone hearing you have gone from abnormal to normal.
[1] These organizations all consider your fasting glucose level and HbA1c, a measure of long-term glucose elevations. They differ in what they feel is a normal range, the cut-offs of concern, and how to combine the measures or not.
Source: Risk of Progression to Diabetes Among Older Adults With Prediabetes JAMA Internal Medicine DOI: 10.1001/jamainternmed.2020.8774

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


