
- 25% of Medicare beneficiaries reported “difficulty affording medications” in 2019
- 16.8% of adults do not take their medications as prescribed or at all
- “Price increases are associated with fewer patients filling their drug prescriptions, regardless of health risks or the number of drugs prescribed.”
With this background, researchers set out to look at the hypothetical costs to a patient for medically managing their chronic illnesses according to our best treatment guidelines. They wondered whether the institution of Medicare’s Part D prescription drug program had brought prices down – a reasonable interest given the current push for medication price reform. A sentinel study done before Part D provided out-of-pocket costs for five chronic conditions, so after adjusting for inflation, they had good data for the “before” comparisons.
While the underlying data is quantifiable, those costs were applied to a hypothetical patient receiving medications according to accepted national guidelines. In the cases where the severity of chronic illness lies along a spectrum, e.g., heart failure and elevated cholesterol, and medications are intensified with increasing disease severity, they chose a patient in the middle of the range. Most importantly, they did not consider the additional monthly costs of Part D coverage – roughly $500 annually, or the discounts that some lower-income beneficiaries can receive. [1] These are costs at the spectrum's lower, but not the lowest end.
The researchers considered the eight most frequent chronic conditions across fifteen classes of medications, in 2009, that included 47 medications; by 2019, 58. The outcomes were broken out by each disease and two “clusters” of chronic illness – let’s ignore the clusters and look at individual costs. I’ve stripped the table of the numbers to focus on the changes.
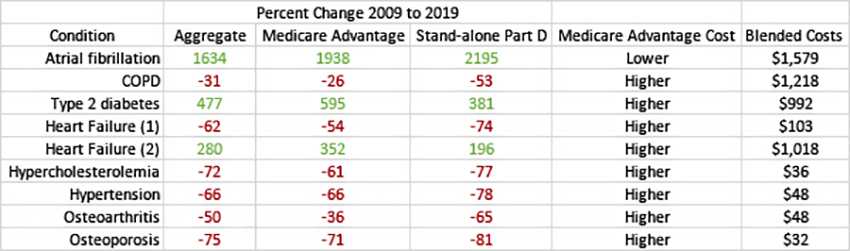
All the findings are statistically. Part D programs are broken out into those associated with Medicare Advantage Programs and programs purchased by those using traditional Medicare [2]. The second-to-last column reflects the actual out-of-pocket costs to the beneficiaries, comparing Medicare Advantage to stand-alone coverage.
- Except for three conditions, costs came down.
- Despite the cost reduction, Medicare Advantage beneficiaries paid greater out-of-pocket costs than those with stand-alone coverage.
- While it is not shown in the table, the institution of Part D coverage did result in lower out-of-pocket costs for beneficiaries since 2004. When adjusted for inflation, these out-of-pocket costs required only 6.7% of a beneficiary’s income compared with 20% in 2004.
Why do some costs rise and others fall?
In the instances where costs fell, we are looking at common conditions best treated with medications with generic options. When guidelines recommended medications without generic alternatives, the cost increased substantially from 3 to 16 fold. Those rising costs come from a new generation of medications being recommended, as the researchers write,
“Moreover, as new evidence has been generated suggesting improvements in clinical outcomes associated with these drugs, including evidence to support their use for other indications, they have been increasingly prescribed.” [emphasis added]
You’ll note the phrase "suggesting improvement." In a sense, we are paying more for medications that have yet to be shown to be “worth” the price increase. This is due, in part, to the approval of drugs by the FDA based on “non-inferiority” studies, where medication is found to be equivalent to ones already in use. Britain’s National Institute for Health and Care Excellence (NICE) program determines their medication options. They include a consideration of value, whether the medication is better than what is already available. There are many ways to assess value, ease of access, administration, improvement in outcomes. So consideration of “value” does not guarantee that a “me-too” drug will not be approved. It is just an explicit consideration, something we might emulate here.
“…our base-case analyses suggest that proposed pricing for aducanumab as has been stated by the manufacturer would not be in alignment with its clinical benefits.”
 This is the conclusion by NICE for Aduhelm, Biogen’s Alzheimer's medication that has caused such a furor over its costs and benefits. You can read the NICE determination here; while you may or may not disagree with them, they are explicit and stated before a decision is made.
This is the conclusion by NICE for Aduhelm, Biogen’s Alzheimer's medication that has caused such a furor over its costs and benefits. You can read the NICE determination here; while you may or may not disagree with them, they are explicit and stated before a decision is made.
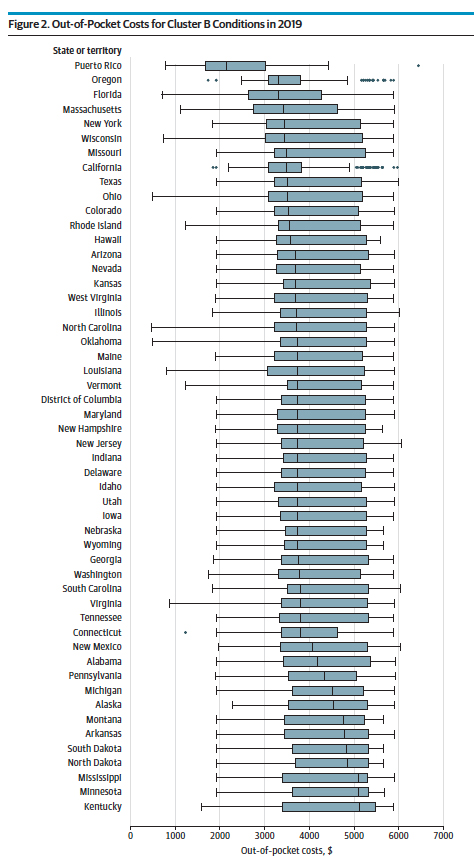
Let me end with two more quick thoughts. First, consider the graphic at the left that shows the out-of-pocket costs for the aggregate of those chronic illnesses – and it does include those far more expensive treatments for heart failure. But if you look at the median out-of-pocket costs, the dark line in the box see how it changes from a low in Puerto Rico to a high in Kentucky. What is that health inequity about?
Second, Medicare Advantage programs make a big push for enrollment in December – we just survived the onslaught of the “Call now for your additional benefits” advertisement. But how is a knowledgeable consumer expected to choose a plan based upon costs hidden in the wording? Except for atrial fibrillation, beneficiaries' out-of-pocket costs in Medicare Advantage were higher than stand-alone Part D coverage. Where is the bargain? Perhaps we should have an app that looks at our yearly spending and tells us what it is projected to cost in the next year across all the choices – then maybe, those ads would have some real value to patients.
[1] That number is taken from this source; if you spend a few moments reading the rest of the information, you will realize how confusing the cost of medications is to Medicare beneficiaries
[2] Medicare Advantage takes on all of traditional Medicare costs at a monthly premium, restricting the choice of physicians and hospitals to “in-network,” but providing perks for dental, eye, and other coverage.
Source: Assessment of Hypothetical Out-of-Pocket Costs of Guideline-Recommended Medications for the Treatment of Older Adults With Multiple Chronic Conditions, 2009 and 2019 JAMA Internal Medicine DOI:10.1001/jamainternmed.2021.7457

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.

