
Who are these people?
Right away, we are in trouble because a definition is not readily at hand. Perhaps we can go with transgender people experiencing “their gender identity as different from the sex which was assigned to them at birth.” Sex commonly refers to our biological phenotype; gender is more our social identity. When one gender transitions, they seek to align their phenotype with their social identity. While there are federal and state regulations regarding redesignation in legal documents, how to handle these transitions in medicine in our treatment records is not as well defined.
![]() Transgender individuals may maintain their biologic phenotype or seek to alter it with hormonal therapy, surgical intervention, or both. From the point of view of treating an individual, there are distinct differences promoted by our hormones, so how can we alter the demographics of our medical records to reflect this critical information?
Transgender individuals may maintain their biologic phenotype or seek to alter it with hormonal therapy, surgical intervention, or both. From the point of view of treating an individual, there are distinct differences promoted by our hormones, so how can we alter the demographics of our medical records to reflect this critical information?
As reported in the Journal of the American Medical Informatics Association, the CDC has adopted the method to the left. I personally find transmale less clear than female-to-male (FTM), but at least it allows physicians to recognize the presence of an altered hormonal milieu.
Additionally, medical records capture our preferred names, e.g., how I wish to be spoken to, so that may explain why we begin to see preferred pronouns in correspondence – and those pronouns can be male, female, neutral (“they”), or we may wish not to be referred to by pronouns at all.
Transgender’s Recent History
Transgender individuals have been around forever. But rather than attempt to identify famous individuals in our distant past, let’s pick up the story with Dr. Harry Benjamin, a German physician visiting the US in 1913 to learn about, as it turned out, a quack treatment for tuberculosis. On his voyage home, he was caught “mid-Atlantic both by the outbreak of the First World War in 1914, and the Royal Navy.” He chose to return to the US rather than a British internment camp, opening a practice initially in New York and later in San Francisco.
"Look at this boy, he's not a boy! You've got to do something to help my son be a girl!"
In 1948, this boy, actually 23, was referred to Dr. Benjamin by his good friend, Dr. Alfred Kinsey (yes, that Dr. Kinsey). He was treated with estrogen with a good response and ultimately underwent gender reassigning surgery in Germany. Dr. Benjamin coined the first word for this condition, transsexualism, which remains today a codable, that is billable, diagnosis. His more famous patient was Christine Jorgenson, who underwent a “sex-change” operation that began in Denmark and ultimately was completed in the US. Jorgenson was credited with bringing the transgender community its first national attention.
In 1963, Dr. Milton Edgerton set up the first gender identity clinic at Johns Hopkins, primarily treating complications from gender-altering surgery performed outside of the US. Although plagued by many surgical complications, Dr. Edgerton wrote, “not a single patient regretted having had the original surgery.” In 1969, one of Dr. Benjamin’s patients funded the” first international symposium on gender identity,” which led to the creation of the World Professional Association of Transgender Health, which remains an essential source of guidance in the healthcare of transgender individuals.
The Transgender Community
It is hard to describe the total population of transgender individuals. Estimates range from 0.4 to 1.3% of the global population.
The 2008 National Transgender Discrimination Survey of over 7,500 self-identified transgender individuals from all 50 states, the District of Columbia, Puerto Rico, and our territories offer some additional information. While more recent studies show slightly different numbers and percentages, these will get you in the ballpark.
Among the respondents:
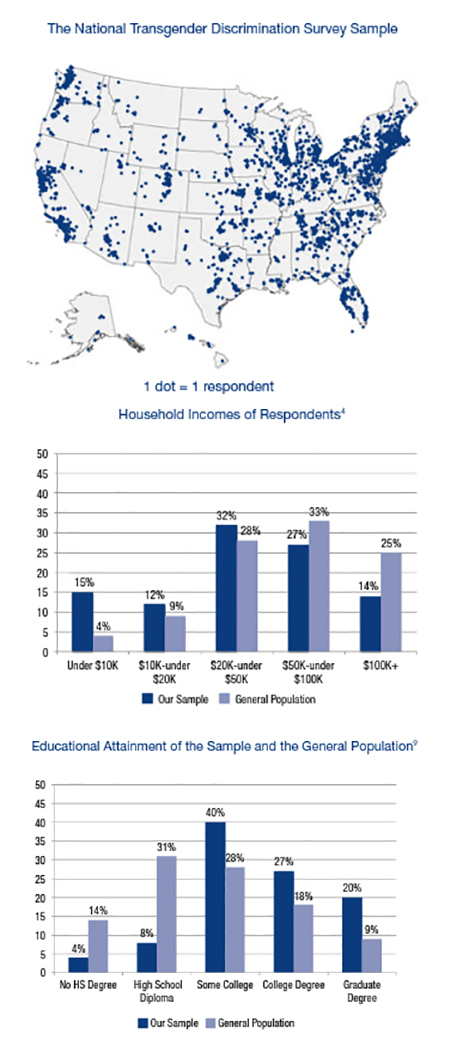 76% were White, 5% Black or Latino, 2% Asian, 1% Indigenous Natives, and 11% multi-racial
76% were White, 5% Black or Latino, 2% Asian, 1% Indigenous Natives, and 11% multi-racial- 19% were age 18-24, 53% 25-44, 17% 45-54, 11% 55-64, and 2% over 65 years of age
- 70% were currently employed, 11% were unemployed, and 19% were out of the workforce.
- 30% reported a physical disability or mental health issue (compared to 20% in our general population)
- 55% lived “full-time in a gender different from their birth sex.” 27% lived part-time in a different gender but aspired to a full-time transition.
- Of those who transitioned, 61% had hormonal treatment, 33% additional surgical intervention.
- Most transitioned between the ages of 18 and 44. Female-to-male transitions occurred earlier (18-24) than male-to-female transitions (25-54)
- 89% were registered voters (as compared to 71% at the time of the 2008 election)
- 20% were or had been members of the armed forces (as compared to 10% of the adult population at that time)
A more recent study from 2016 looked at transgender Medicare beneficiaries. There are significant numbers within Medicare’s ranks based on disability rather than age. 84% in this sample of roughly 4100 beneficiaries. The researchers believed that limitations in their methodology to identify these beneficiaries resulted in underestimation. These individuals have significant co-morbidities
![]()
Most specifically, mental health issues and tobacco and drug use disorders. The beneficiaries over 65 also had more significant hypertension, cholesterol issues, coronary artery disease, obesity, and diabetes.
Gender Affirming Interventions
The two therapeutic options are hormonal with or without surgical intervention. Let’s begin with hormonal manipulation. Hormones by themselves will “have a profound effect on secondary sex characteristics and psychological well-being.”
- Female-to-male transition utilizes testosterone therapy which alters the presence and distribution of body and facial hair, increases muscle mass and typical male fat distribution. It leads to a cessation of menses, clitoral enlargement, and a deepening of the voice. It can adversely result in elevated red blood cells and a worsening lipid profile.
- Male-to-female transition has two hormonal goals. First, to reduce testosterone levels, either by removing the testicles (orchiectomy) or using anti-androgens, typically an old-line diuretic, spironolactone. Second, exogenous estrogens enhance feminization, which leads to more female fat and hair distribution, diminished muscle mass and libido, and breast growth. Adverse reactions include a higher incidence of deep vein thrombosis and osteoporosis, a loss of bone density.
Many transgender individuals pursue surgical intervention. Typically, those individuals are treated for a minimum of one year with hormonal therapy before a referral is made. [2] In a study of 386 transgender individuals in the Netherlands, 77.3% of male-to-female transitioners and 57.5% of female-to-male transitioners requested hormonal and surgical therapy. Those choosing “partial surgical management” usually opted for hormonal therapy with breast augmentation or mastectomy with or without hysterectomy, as the case indicated.
The reason individuals chose partial therapy was bifurcated. For female-to-male transitioning, the overwhelming concern was surgical risk and outcomes rather than a lack of “an underlying desire to have a phallus.” For male-to-female transitioners, where surgical intervention was less complicated, the primary motive “was the absence of experiencing genital dysphoria or feeling that genital surgery was unimportant or unnecessary.”
- In female-to-male transitions, surgery involves reconstruction of the chest and genitalia. Chest reconstruction, “top surgery,” involves subcutaneous mastectomy, repositioning of the nipple, and in some instances, liposuction to further contour the chest. Genital reconstruction, “bottom surgery,” initial involves the removal of the uterus, ovaries, and fallopian tubes. The construction of a “neophallus” follows. These procedures are complex, requiring the combined effort of plastic, gynecologic and urologic surgeons; and often complicated (40%) by strictures or fistulas (abnormal connections) of the urethra, the tube carrying urine from the bladder to the outside. Successful surgery allows for urination while standing and a sensate neophallus capable of some degree of vaginal penetration.
- In male-to-female surgical transitions, top surgery involves breast augmentation. Bottom surgery involves “penile disassembly and inversion.” Like its counterpart, it is frequently complicated by urethral difficulties resulting in incontinence, recurrent bladder infections, and dyspareunia – pain upon intercourse.
Depending upon the voice changes associated with hormonal treatment, additional procedures can be performed to reduce the size of the vocal cords and reduce the prominence of the thyroid cartilage, the “Adam’s apple.”
Much has been made in the media about individuals undergoing hormonal or surgical therapy below the age of consent. The gender identity of children fluctuates over time, with typically only 20% or so persisting in a belief that they are of another gender. But adolescents, mid-teens, “who identify as transgender overwhelmingly describe themselves as transgender as adults.” This is the group that has raised the most concern.
On the one hand, some believe that “prevention of secondary sex characteristics of their natal gender” helps reduce their unease. They point to the reversibility of endocrine suppression therapy, arguing that it gives these individuals “time to explore the nature of their GD [gender dysphoria] and gender identity.” Of course, the added recommendation that this therapy is initiated early in puberty [3] raises concerns about their ability to give truly informed consent.
Gender affirming surgery, with rare exceptions, is delayed until the individual is of legal age to make their own decisions.
A more recent study of gender affirming surgery using the National Inpatient Sample (NIS) was reported in 2016, covering 2000 to 2014. The NIS is a statistical sample reflecting 95% of hospital admissions. They identified 37,827 admissions associated with the code of transsexual or gender identity disorder (dysphoria). 40.5% were mental health admissions. Roughly 11% involved gender-affirming surgery. This would be an underestimate because many chest surgeries can be done as an outpatient and are not recorded.
The bulk of those patients undergoing surgery was for genital “bottom” surgery. The trend was for more men than women to initiate surgical intervention. These patients were predominantly from the Northeast and West. Private insurance paid roughly 45% of claims, while self-pay declined over time to about 40%, the difference made up by Medicare and Medicaid. The average hospital stay was three days, with no operative deaths.
[1] Ngram Viewer
2] The general recommendation is that candidates for chest reconstruction provide one letter of referral, while those considering genital surgery provide two letters. It is further suggested that these letters include a psychosocial assessment, a history of the relationship between the patient and referring physician, a statement that informed consent has been obtained from the patient, and that the mental health professional is “available for coordination of care.”
[3] As with most medicine, there is a classification of the phases of adolescence, the Tanner Stages. Hormonal manipulation is felt to be best initiated at Tanner Stage 2 when pubic hair is “downy,” breast tissue begins to be palpable in females, and testicles are larger than an inch in males.
Sources: Electronic medical records and the transgender patient: recommendations from the World Professional Association for Transgender Health EMR Working Group Journal of the American Medical Informatics Association DOI: 10.1136/amiajnl-2012-001472
Harry Benjamin's First Ten Cases (1938-1953): A Clinical Historical Note Archives of Sexual Behavior
The Role of Surgery in the Treatment of Transsexualism Annals of Plastic Surgery
What Surgeons Need to Know About Gender Confirmation Surgery When Providing Care for Transgender Individuals A Review JAMA Surgery DOI: 10.1001/jamasurg.2016.5549
Injustice at Every Turn A Report of the National Transgender Discrimination Survey National Center for Transgender Equality and the National Gay and Lesbian Task Force.
Identifying the Transgender Population in the Medicare Program Transgender Health DOI: 10.1089/trgh.2016.0031
Partial Treatment Requests and Underlying Motives of Applicants for Gender Affirming Interventions International Society for Sexual Medicine DOI: 10.1111/jsm.13033
Temporal Trends in Gender-Affirming Surgery Among Transgender Patients in the United States JAMA Surgery DOI: 10.1001/jamasurg.2017.6231

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


