Is sticking your finger down your throat a pleasant experience? (Sorry, bulimics excluded)
How about sticking it down there and leaving it for three weeks? This is not a gag (sorry).
Thanks to the geniuses at the DEA, if you're a COVID-19 victim in an ICU hooked up to a ventilator with a hard plastic endotracheal tube the width of your finger stuck in your throat it's pretty safe to conclude that your life genuinely sucks.
But things can always get worse. In a humane world, when you're on a ventilator you are out like a light (1) during a power outage. So, if you're properly sedated and someone tosses you into a bubble bath with Kim Jong-un (although this is admittedly unlikely) you'll be none the wiser. You might even think you're enjoying it.
Photos: Days of the year, Medscape, IMDB
And if you happen to be a COVID-19 victim who is unfortunate enough to be in a hospital that has run out of fentanyl, a bath with stinky ol' Kim may not seem like such a bad choice compared to the alternative. This is because all the other stuff aside, endotracheal tubes are very painful. Which is why fentanyl is usually part of the cocktail of drugs used to keep people comfortable (and usually unconscious) during the time that they are attached to the ventilator.
Before we proceed...

HUH? The US has run out of fentanyl?????
Bear with me for a moment while I explore the existential aspects of this.
- As I've written a bazillion times before, although pills like OxyContin were responsible for the surge in addiction and deaths until 2010 when abuse-resistant OxyContin replaced the original formulation heroin immediately became the main driver of opioid-related deaths.
- Three years later, fueled by the unprecedented demand for heroin, illicit fentanyl, which is far more dangerous, began to pour into the country. It was made in labs in China and smuggled into the US through Mexico. From that point on fentanyl became the drug that was responsible for the majority of overdose deaths in the US (2). It still is.
- Now illicit fentanyl (and its analogs) kill twice as many people as heroin.
- But there's a fentanyl shortage.
The "timeline" that follows is almost hilarious. It begins in 2013.
- 2013 - Fentanyl (illicit) starts coming into the US from China.
- 2013 - present. Lots of people die. Way more than before.
- 2017 - In response to tens of thousands of deaths from ILLICIT fentanyl, the geniuses at the DEA decide to cut the manufacture of pharmaceutical fentanyl because...who knows? Pharmaceutical fentanyl contributes just about zero to the total death toll from the drug when compared to street fentanyl.
- December 2019 - (nice timing there) the DEA cuts production by another 31%.
- February 2020 - Two months later another threat – this time a virus – comes in, once again, from China. A whole lot of people get very sick, many of whom need to be on ventilators.
- Now - Some of them suffer needlessly because of a fentanyl shortage (kill me) in hospitals. (Figure 1) This is analogous to not being able to find radioactive debris in Chernobyl.
- The DEA, in all its beneficence, decides to allow companies to make 15% more fentanyl to address the shortage. Small increases in the production of morphine and hydromorphone are also permitted.
- Too little too late. Hospitals are scrambling to find combinations of drugs to keep intubated patients comfortable. (3)
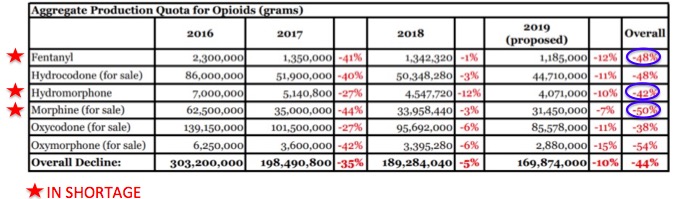
Figure 1. a) Reduction in opioid manufacturing quotas mandated by the DEA. Note the ~50% reduction in quotas from 2016-19 (blue circles). Source: DOJ Office of Public Affairs b) Current shortages of injectable hospital drugs (red star) as reported by the FDA. c) Duh.
Well, at least the three-year 48% reduction in the manufacturing of pharmaceutical fentanyl resulted in fewer deaths from the drug...
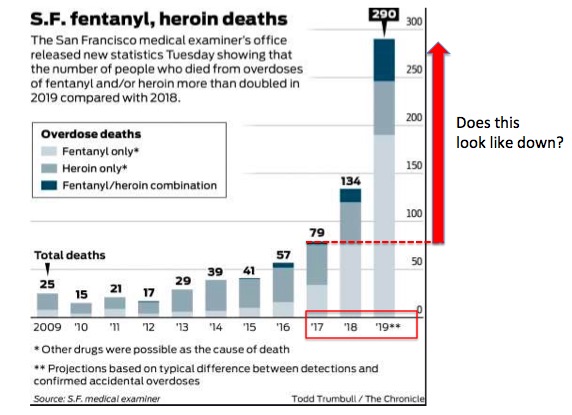
...or maybe not, at least in San Francisco. And across much of the rest of the country as well. Source: SF Chronicle
Although some people are OK with intubation without drugs I am not one of them. I would rather have a swordfish embedded in my eye (which happens more often than you'd think). I will be kicking and screaming. And, unfortunately for any male doctors that may be in the vicinity, I just took (and passed with flying colors) an online course called "Gonad Kicking 101" given by Queens College, the alma mater of "Gonad Emeritus" Andrew Kolodny, who is as responsible for the fentanyl/morphine shortage as any gonad out there.
No, I'm not really cool with being awake while on a ventilator. And I'm not alone. Some random quotes from all over the place:
"Then, I felt as though my body was going into convulsions as gag and cough reflexes were triggered. My eyes teared up, and it felt as though my insides were being “pulled out."
"[The patient] is constantly exposed to the hissing sound of the ventilator and sounds from alarms on IV pumps, cardiac monitors, and ventilators. The suction catheter threaded through the endotracheal tube stimulates a cough and gag reflexes, and leaves her gasping for air at times."
(From a physician) "It’s torture to have someone awake on the vent but sometimes MDs want them off sedation for a time to assess neuro status. Trust me it is never peaceful. No one is smiling."
"It’s weird how most people aren’t totally calm and cooperative when they feel like they’re constantly gagging on a tube that’s simultaneously forcing air into them and also not letting them catch their breath."
Lovely.
Once again folks, our government at its finest. I'll withhold my opinion of our handling of the coronavirus pandemic, but our drug policies, which were plenty bad before the virus hit have now reached a new level of ineptitude.
Let's close with some good wishes to Physicians for Responsible Opioid Prescribing (PROP), a group of [I'm not allowed to use this word. You fill it in] whose anti-opioid madness has caused a decade of misery for pain patients and now extra problems for COVID patients. Shove that down your throat, guys. Or wherever.
NOTES:
(1) Some patients actually prefer to be conscious while on a ventilator. This I don't get. I guess some people like chewing on glass too.
(2) See The Opioid Epidemic In 6 Charts Designed To Deceive You
(3) In an example of pure madness, fentanyl, midazolam, vecuronium bromide, and rocuronium bromide, which are all important for pain control, muscle paralysis, and sedation during intubation are all in short supply. One reason, recently discussed in Slate is that these same drugs are used for lethal injections and are being hoarded by states that have capital punishment. Yes, hanging on to death penalty drugs while these same drugs are needed to treat COVID patients. I'll let the medical ethicists grapple with that one.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.

