There is an urgent need to evaluate immune response kinetics with the aim of monitoring vaccination coverage. [1]
The critical consideration – do the rates of new vaccinations exceed attenuation rates of previous immunization, based on published rates of vaccination and assumed attenuation rates? We based our analysis on 2021 population-based trends in the administration of primary and booster vaccines [2], comparing rates of increasing population protection with rates of attenuation over time. We proposed attenuation scenarios involving selected rates of such losses and compared their effects on vaccination status with and without booster shots. All of this is hypothetical; we considered no outcome data, and our operational mantra is, “What if?”
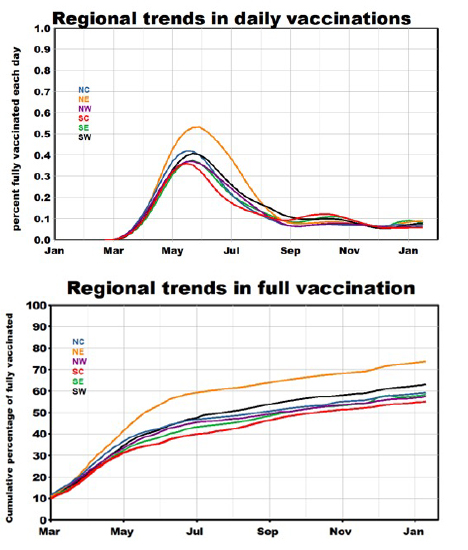 Regional primary vaccination rates have been essentially similar with the highest rates in the Northeast. Daily vaccination rates rose among regions from January through March, peaked in April, and then declined 3-fold with essentially constant rates after that. We see no indications of recent upticks. Cumulative rates increased steadily at about 1% per week after June, reflecting the higher peak in the Northeast’s daily rates. These parallel trends suggest that any underlying regional differences have remained constant throughout the pandemic. We limited our attenuation analysis to the Northeast and South Central regions for visual clarity. [3]
Regional primary vaccination rates have been essentially similar with the highest rates in the Northeast. Daily vaccination rates rose among regions from January through March, peaked in April, and then declined 3-fold with essentially constant rates after that. We see no indications of recent upticks. Cumulative rates increased steadily at about 1% per week after June, reflecting the higher peak in the Northeast’s daily rates. These parallel trends suggest that any underlying regional differences have remained constant throughout the pandemic. We limited our attenuation analysis to the Northeast and South Central regions for visual clarity. [3]
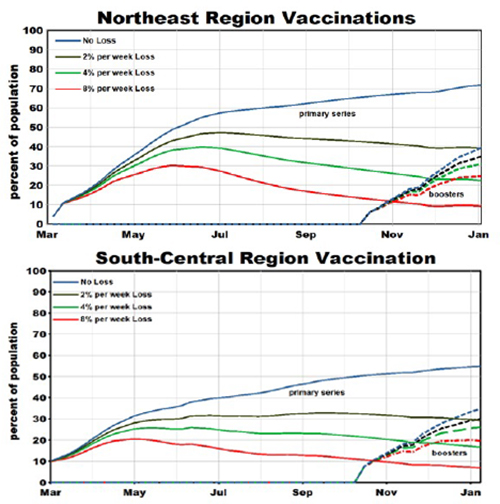
We developed an algorithm in which protection from the virus is progressively attenuated at a constant monthly rate. We selected nominal rates of 2%, 4%, or 8% to demonstrate the resulting trends. Each week, those who were vaccinated defined a cohort for which attenuation was estimated and summed over the pandemic to estimate cumulative effects. Booster shots are restricted to those who had completed the primary series.
 Attenuation effectively increases the “unvaccinated” by about 25 percentage points per attenuation rate percentage. This gap could only be lessened by increasing the rate of primary vaccinations above the current rate of about one percentage point per week.
Attenuation effectively increases the “unvaccinated” by about 25 percentage points per attenuation rate percentage. This gap could only be lessened by increasing the rate of primary vaccinations above the current rate of about one percentage point per week.
Primary vaccination separates a population into two subsets. Protection of the vaccinated subset can be maintained utilizing booster shots; failure to do so effectively increases the unvaccinated share of the population. In any event, adequate protection of a population depends on the rate of primary vaccination and limiting the attenuation of the vaccinated.
Effective primary protection rates declined after June in the Northeast, less so in South Central. There was essentially no difference between the regions for 4% or greater attenuation rates. In these models, 50% attenuation of vaccine effectiveness occurred after 8, 4, and 2 months for 2%, 4%, and 8% attenuation rates, respectively.
Booster shots are intended to offset the attenuation of the primary vaccinations. We added the primary and booster rates to evaluate the likelihood of achieving adequate protection. This could be accomplished in mid-January if attenuation rates are <2%/week, slightly higher in South Central. Had the attenuation rate been higher, earlier administration of booster shots would have been required, and the overall protection rate (primary + booster) would have been lower.
A simplifying assumption of our algorithm is that each vaccination is equally effective for the population during the pandemic, imparting a similar measure of virus protection to the population. Diminished protection would follow suit as vaccine effectiveness waned over time. We realize that these assumptions may well be unrealistic for reasons beyond the scope of this simple analysis. Nevertheless, these simulated scenarios are intended to introduce duration as an essential characteristic of a vaccine, in addition to efficacy.
Reducing vaccine attenuation may be as important as converting recalcitrant first-time vaccinators.
[1] IgG antibodies against SARS-CoV-2 decay but persist four months after vaccination in a cohort of healthcare workers Clin Chim Acta DOI: 10.1016/j.cca.2021.10.035
[2] Daily rates of COVID vaccinations are from the CDC.
[3] The states included are Connecticut, Delaware, Maine, Massachusetts, New Hampshire, New Jersey, New York State, Pennsylvania, Rhode Island, and Vermont for the Northeast Region, and Kansas, Louisiana, Missouri, Oklahoma, and Texas for the South Central Region.


