
The study reported in JAMA Network Open looked at 314,763 patient visits involving 42% non-Hispanic Whites, 33.8% non-Hispanic Blacks, and 21.1% Hispanics.
First-come, first-served
Emergency Departments (ED), given the wide range of what is considered an emergency, are never first-come, first-served. Patients are prioritized by a five-level Emergency Severity Index (ESI). A trained “triage nurse” estimates the resources necessary to treat patients based on their vital signs, symptoms, and personal observations and assigns an ESI score. Level 1 patients require immediate care, 2’s and 3’s attention within 15 minutes, and level 4 or 5 care within 30 minutes. Roughly two-thirds of EDs use the system, although, to be fair, given the significant increases in ED visits, those time frames rarely apply.
Patients are placed in line to be seen based on their ESI score and within that scoring on the arrival time – a semi-first-come, first-served algorithm.
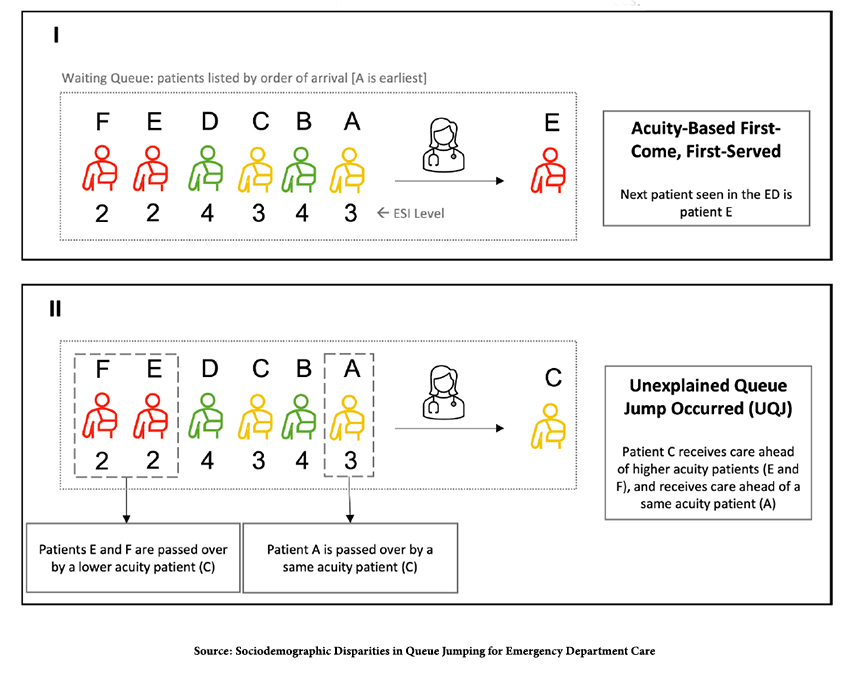
But sometimes the ordering of patients is changed, an unexplained “queue jump.” Jumping the line are patients taken later than their line position jumped over by patients with lower acuity (ESI level) or the same acuity but later arrival time.
The outcomes of interest were on the effect of those care delays
- Placement in ED hallways rather than rooms
- Leaving without completion of care
- Subsequent return to the ED within 72 hours
- Care escalation is the admission to a unit with higher level care than initially ordered.
Data Points
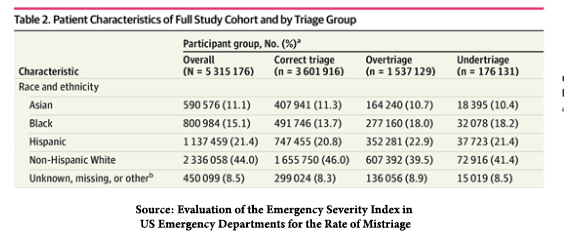
There were no disparities in those considered most urgent, ESI level 1. And it is impossible to be jumped over in ESI 5, basically individuals using the ED for primary care needs. The analysis only considered ESI levels 2-4 – the categories with nearly 98% of patients, making it a poor discriminator. In a similar but more extensive study by Kaiser Permanente undertriage, those jumping the line occurred 3% of the time; over triage, those being jumped occurred roughly 28% of the time. [1]
- 53% of all patients were cared for in the “correct” order – no line jumping
- 28% were passed over by a patient with a lower acuity or having arrived later. The remaining 22% were those jumping patients.
- Generally, arrival time within an ESI grouping was the most common “queue violation.”
You were more likely to be jumped over if you
- Used Medicaid as your primary insurance, 11%
- Were non-Hispanic Black, 5% or Hispanic, 5%
- Used Spanish as your primary language, 6%
- Gender played no role.
For those being jumped over
- 3% left the ED without completing their care, although there were no higher rates of ED return within 72 hours.
- 1% were most likely to be placed in a hallway bed. Those hallway placements were far more likely to reflect the same acuity and later arrival times than acuity jumps.
- There was no care escalation.
If you are a numbers person, it appears that being poor, Black, or Hispanic, at least presumably in the New Haven area, it is a Yale study, you may be jumped over for care by others. If you are a clinician, the only clinical consequence to these patients being jumped over is that they left without completing their care. But they didn’t return to the ED at higher rates than those treated in order.
Why might one group be jumped over more than another?
“Mechanisms of structural racism and classism could explain our observation that minoritized racial and ethnic groups and patients who were uninsured or relied on public insurance were more likely to experience disadvantageous queue violations (higher odds of being passed over and lower odds of receiving care ahead of others) than privately insured White patients.”
The statement could explain those disparities, but is a bold way to begin a discussion and suggests a preconceived bias. And while I applaud the researchers for adding the social construct of class to the mix, their metric, uninsured or public insurance, the factor exhibiting the most substantial effect, more than twice the impact of race, is not known at the time of triage, so that can’t be a direct variable in prioritization.
They go on to consider and detail various underlying institutional and personal sources of racism. It is only under limitations that other possible causes of line jumping are considered.
There is no explanation for why patients were jumped. Certainly, a worsening severity of illness while waiting is a clinically appropriate reason to jump the line. And we do not know whether family members were advocating for being seen. More importantly, we do not know the race of those jumping. Is it racist for a black patient to jump over another black patient, or must they be Hispanic or White?
Other factors determine whether you jump the line, including how you arrive in the ED. Those arriving by ambulance do not go to the waiting room, irrespective of their ESI. 48% of patients arrived as transfers or by ambulance and were automatically possible line jumpers. The fact that many of the “queue violations” were the same severity later arrival suggests this is a significant source of the disparities.
Then we must consider the mix of patients presenting to the ED and the staffing level. Both were “controlled” in the researcher’s statistical analysis but to what degree? Take, for example, the “poorer” outcome of hallway bed placement. The majority of those individuals were jumped by the same acuity later arrivals. That suggests there was a need for a private room for the patient doing the jumping, which is not an uncommon problem in the presence of an infectious disease or mental health issue.
This study demonstrates, at best, as did the Kaiser Permanente study, that while we may more accurately identify the appropriate triage category for Whites, we under and over-triage patients to the same degree when it is categorized by race.
 There is no doubt that human-designed systems of prioritization make mistakes. And it is essential to try and improve them. But using the social constructs of race as the sole discriminator or the latest dog whistle buzzword, disparity, does not serve us well – unless you want to jump the line for publication.
There is no doubt that human-designed systems of prioritization make mistakes. And it is essential to try and improve them. But using the social constructs of race as the sole discriminator or the latest dog whistle buzzword, disparity, does not serve us well – unless you want to jump the line for publication.
[1] They found that only 1% of Hispanics were under or over-triaged. For Blacks, 18% were undertriaged, 5% over triaged. Having a non-English primary language was associated with about 4% less under or over-triage.
Source: Sociodemographic Disparities in Queue Jumping for Emergency Department Care JAMA Network Open DOI:10.1001/jamanetworkopen.2023.26338
Evaluation of the Emergency Severity Index in US Emergency Departments for the Rate of Mistriage JAMA Network Open DOI: 10.1001/jamanetworkopen.2023.3404

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


