In a recent comment to an article on an ACSH article titled “Can a ‘Superopioid’ Treat Pain Without Opioid Baggage? A Nature Paper Says Maybe,” a reader asked a pointed question: What happens if a patient on chronic opioid therapy does not experience euphoria? The commenter highlighted a common misunderstanding in public and policy debates, that opioids primarily deliver a recreational “high” even when used long-term for legitimate pain management. This question cuts to the heart of a critical distinction too often blurred in discussions of the opioid crisis: the difference between physical tolerance and addiction, and between analgesia for suffering patients and the reward-seeking behavior that drives misuse.
Tolerance to Euphoria Is a Well-Documented Pharmacological Reality
Scientific literature consistently shows that many patients on stable, long-term opioid regimens for chronic pain report little to no euphoria after the initial period of use. Tolerance develops to the euphoric (and often sedative) effects of opioids, frequently more rapidly or prominently than to other effects. Neurobiological adaptations in the brain’s reward circuitry—particularly dampened dopamine signaling in the mesolimbic pathway—shift the motivation for continued use away from pleasure-seeking toward avoidance of withdrawal-related dysphoria or simple maintenance of pain relief.
The following graphic illustrates this dose-response relationship in a simplified but informative way:
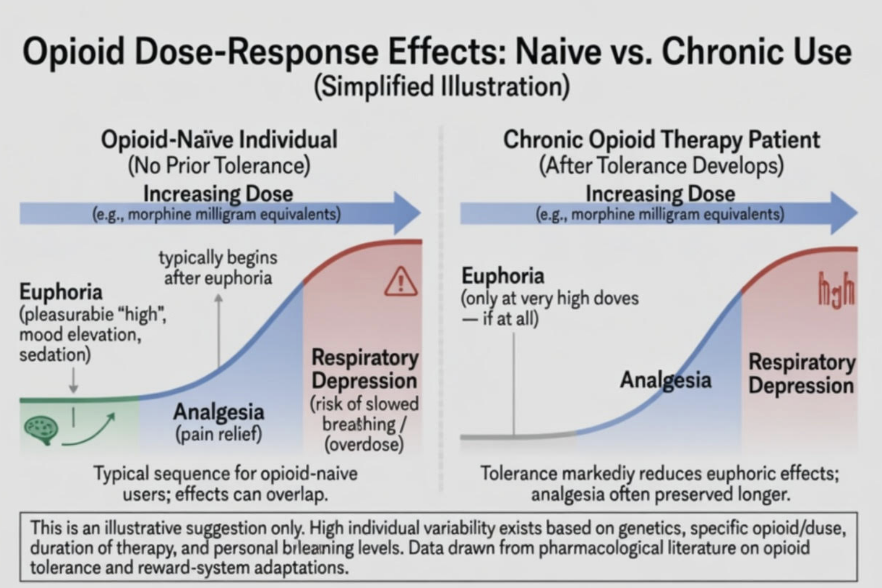
As shown, in opioid-naïve individuals, euphoria often emerges at relatively lower doses, followed by analgesia, with respiratory depression occurring at higher doses. In contrast, after tolerance develops with chronic use, the euphoria threshold shifts dramatically to very high doses, while analgesia can often be achieved at more moderate (though still elevated) levels. This illustration emphasizes the high individual variability influenced by genetics, specific opioid and dose, duration of therapy, and level of tolerance.
In my clinical experience treating patients with chronic pain, I have observed this trajectory in the great majority of adherent patients on long-term opioid therapy. Once stable dosing is established, most no longer report euphoria that may have been noticeable early in treatment. Instead, they describe the medication as enabling better function, improved sleep, and relief from the exhausting burden of unrelenting pain without the intoxicating “high” commonly assumed by the public.
Separating Pain Patients from Addiction Narratives
Failure to recognize this distinction has real-world consequences. Many chronic pain patients, estimated in the millions in the U.S. rely on opioids for functional improvement when other treatments fall short. Studies of long-term opioid therapy in carefully selected patients show variable but sometimes sustained benefits in quality of life when doses remain stable and monitoring is appropriate. Yet policy responses that emphasize “opioid baggage” (respiratory depression, dependence, misuse potential) have sometimes led to abrupt tapers or denials of care, leaving patients in untreated agony.
These same neuroadaptations help explain a dangerous pattern seen in severe opioid use disorder (OUD). Individuals with severe OUD (addiction) who continue to chase the euphoric “high” must escalate to increasingly higher doses because tolerance has blunted the reward response. Often, they reach or exceed the dose range that induces respiratory depression, dramatically elevating overdose risk. This stands in stark contrast to most adherent chronic pain patients, who typically maintain stable doses focused on analgesia rather than reward.
Research indicates that the risk of developing opioid use disorder among chronic pain patients prescribed opioids is relatively low—often cited at less than 1 to 8% range depending on definitions and populations, though not zero. Most patients who develop problematic use exhibit behaviors centered on compulsive seeking, loss of control, or continued use despite clear harm, rather than simple tolerance. In contrast, recreational or non-medical users often chase the initial euphoric effects that diminish with tolerance.
A thoughtful analytic review framed motivations for opioid use along a spectrum: analgesia for most pain patients versus euphoria or the search for “oblivion” (escape from emotional distress) in those with severe OUD. It argued that conflating these motivations unfairly stigmatizes legitimate pain management. Extended-release and transdermal formulations further reduce euphoric potential after tolerance is induced by avoiding sharp blood-level spikes.
Implications for New “Superopioids” and Policy
The ACSH article discusses a novel nitazene-derived compound from a recent Nature paper that, in rodent models, provides analgesia with a flatter dopamine response, appearing to limit reinforcing drug-seeking behavior. If such biased or “super” agonists translate successfully to humans, they could further decouple pain relief from euphoria and addiction liability, validating the idea that not all µ-opioid receptor activation produces the full problematic package.
This research echoes the need for nuance. Chronic opioid therapy involves predictable tolerance to euphoria and other effects, but that does not equate to OUD for most adherent patients. Guidelines from pain societies have long stressed individualized assessment, risk stratification, and monitoring rather than blanket avoidance.
Public discourse and policy must reflect this evidence. Overly restrictive prescribing driven by fear of euphoria has contributed to undertreatment of pain, patient suffering, and sometimes shifts to illicit markets. At the same time, vigilance against misuse remains essential. Education for clinicians, patients, and policymakers should highlight that many patients on chronic therapy do not chase or experience a high; their medication enables basic functioning amid debilitating conditions.
The commenter on the ACSH article asked a deceptively simple question that deserves a clear, science-based answer: when patients on chronic opioid therapy no longer experience euphoria, it often signals normal pharmacological tolerance rather than impending OUD. Their continued use typically reflects an ongoing need for analgesia, not recreational reward. Recognizing this reality, supported by both research and clinical observation, could foster more compassionate, evidence-based approaches to pain care that balance risks without abandoning those in genuine need.
Lynn R. Webster M.D. is Senior Fellow Center for U.S. Policy and is co-author of the forthcoming book, Deconstructing Toxic Narratives: Data, Disparities, and a New Path Forward in the Opioid Crisis, to be published by Springer Nature.

Lynn Webster, MD
Lynn R. Webster, MD, is a pain and addiction medicine specialist and serves as Executive Vice President of Scientific Affairs at Dr. Vince Clinical Research, where he consults with pharmaceutical companies.


