
May is Melanoma and Skin Cancer Awareness Month, and while we have missed Melanoma Monday, the first Monday in May, it is not too late to talk about a cancer that has dramatically changed trajectory over the last decade.
A quick primer
Our skin consists of an outer layer, the epidermis, and two deeper layers, the dermis and the fat and connective tissue that help create our contours. That outer layer contains several key cell types, including basal and squamous cells, along with melanocytes, the pigment-producing cells that make melanin. All three can develop into cancers and differ in their behavior.
Basal cell carcinoma is the most common type of skin cancer, growing slowly and rarely spreading. Squamous cell carcinoma, the type associated with chronic sun exposure, is somewhat more likely to spread but remains generally treatable. Melanoma is even more likely to spread and is responsible for most skin-cancer deaths.
Paul Chapman, MD, is the Chief Medical Research Officer for the Meyer Cancer Center at Weill Cornell Medicine and New York-Presbyterian Hospital. He has been an active clinician and researcher focused on understanding and treating melanoma throughout his career, including participation in the first clinical trials of targeted therapy. We got together for a brief discussion, which has been lightly edited.
CD: Melanoma is often described as both highly preventable and potentially deadly. What makes it biologically different from other skin cancers?
PC: It is eminently preventable in the sense that most melanomas are early stage. If detected early, it can be easily removed, and almost all of those patients are cured. That said, some percentage of melanomas spread [to the lymph nodes or organs] before they can be resected, and in a small percentage of patients, they never have a detectable primary melanoma.
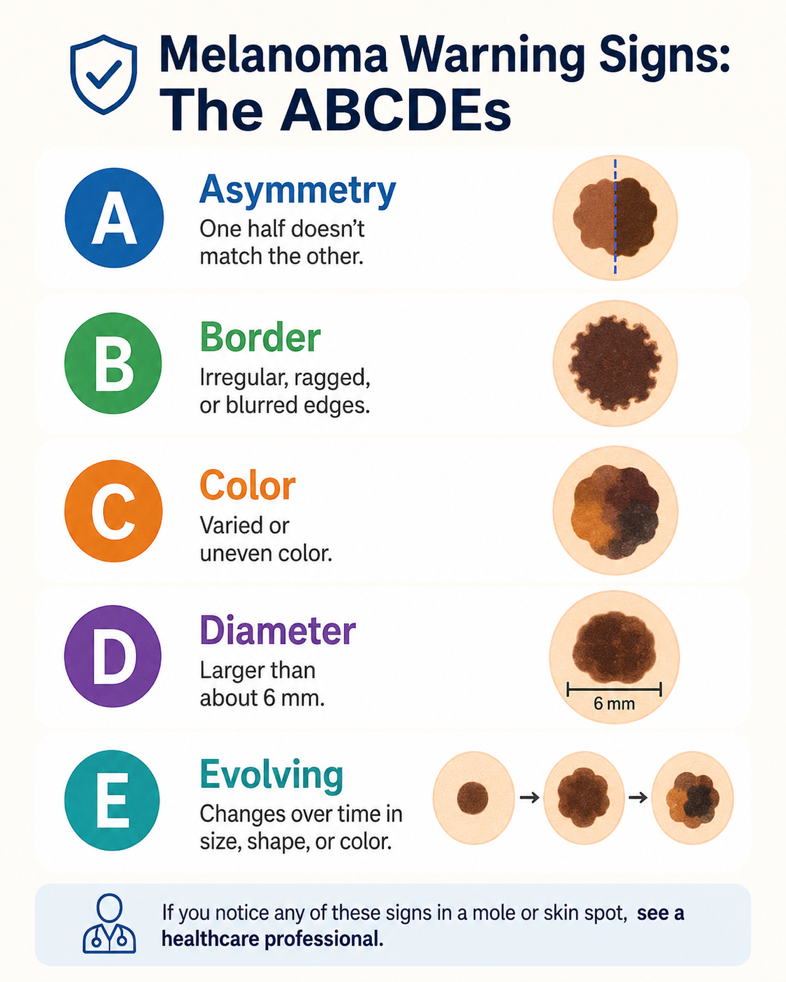 CD: You said it's highly preventable, which, of course, leads to the next question. What do we tell people to watch for, and when should they speak to a dermatologist or a physician?
CD: You said it's highly preventable, which, of course, leads to the next question. What do we tell people to watch for, and when should they speak to a dermatologist or a physician?
PC: Any mark on the skin that is growing, bleeding, or new. Those are lesions that ought to be looked at by a dermatologist and probably removed.
CD: Are there any groups of people who should have annual visits to a dermatologist?
PC: With respect to melanoma detection, patients with high-risk factors should be screened regularly by a dermatologist. This includes people who have lots and lots of moles, people with a previous history of skin cancer, a family history of melanoma, or a history of severe sunburns or chronic sun exposure, including a history of sunbed usage.
CD: Is AI entering detection here?
PC: It is, in the sense that the dermatology world has been trying for a number of years to use AI to assess images of skin lesions to see if AI can learn to distinguish melanoma from benign changes. It turns out that it's not as easy as you might think. This is because photographic techniques can vary quite a bit from patient to patient and from mole to mole, and AI picks up on differences in lighting and background skin color. It's hard to get it really standardized. For lesions that are either clearly melanoma or clearly benign, AI can learn to make that distinction pretty well.
But AI has not been very accurate so far in interpreting the tough lesions that everyone struggles with. I think it's coming, but it's not there yet.
CD: The public hears a lot about sunscreen, protective clothing, shade, and avoiding tanning beds.
PC: There is data on squamous cell cancers and sunscreen. Much of that data has been extrapolated to melanoma, so there isn't any direct evidence for that. However, everyone in the melanoma field strongly recommends the use of sunscreen and protective clothing. There is data on sunbeds, and people who frequent tanning salons have a slightly higher risk of melanoma. I think it's about a one- to twofold higher risk. So obviously, we do not encourage the use of sunbeds.
CD: When I was in medical school, melanoma was pretty much a death sentence. And that's changed dramatically. What do you think has made the most dramatic changes?
PC: Until 2009, chemotherapy was the only treatment, and that's the mortality rate you remember, with the one-year survival rate around 10%. With chemotherapy, we occasionally cured someone, but it was uncommon.
Then, in the early part of this century, two things happened. We discovered that melanomas frequently had a mutation in the gene BRAF [1], and we also learned about immunotherapy using checkpoint inhibitors [2].
Both treatments were reported to yield astounding results, especially compared with what we had before. Over the past 10 to 15 years, we've developed more sophisticated BRAF inhibitor and checkpoint inhibitor therapies. Now the one-year survival rate is somewhere around 60-70%.
CD: Is there any message you want to convey to the general population about melanoma?
PC: I tell all my patients that you don't have to stay out of the sun, but you should not be trying to get a suntan. Don't get a sunburn. Use sunblock. I remind patients that their tanning reaction is their skin detecting DNA damage. That's why you get darker.
And if you see something, say something.
CD: Thank you for your time.
The message is straightforward: melanoma outcomes depend heavily on prevention, early recognition, and timely care. People do not need to avoid the sun entirely, but should avoid tanning and sunburn, use sun protection, and pay attention to new, changing, growing, or bleeding skin lesions. The science of melanoma has changed dramatically, but the practical advice remains simple, as Dr. Chapman says, “if you see something suspicious, say something.”
[1] This mutation acts like a stuck accelerator pedal in a growth-signaling pathway, telling melanoma cells to keep dividing. BRAF-targeted drugs are designed to interrupt that signal. About 40–60% of metastatic melanomas have a BRAF mutation.
[2] Checkpoint inhibitorshelp the patient’s own immune system recognize and attack melanoma cells. Cancer cells can exploit immune “brakes,” or checkpoints, to hide from T cells. Checkpoint inhibitors block those brakes

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


