The old “Dr. Google” era has given way to a faster, louder medical marketplace: TikTok, Reddit, podcasts, and influencer-led telehealth. In that ecosystem, “spermmaxxing” has emerged as a male-fertility spin on optimization culture, promising ways to maximize sperm count, motility, and testosterone. At the same time, viral anecdotes about “Ozempic erectile dysfunction” have fueled anxiety. Both narratives can serve as marketing tools for compounding pharmacies, telehealth subscriptions, and lifestyle guides, making it especially important to separate signal from sales pitch.
As with many social media trends, there is often a kernel of truth at the bottom of the rabbit hole. The maxxing pivot to GLP-1s, away from testosterone replacement therapy (TRT), is net positive because TRT lowers sperm counts. Ozempic ED may or may not exist. Bringing male infertility into the conversation is long past due. The influencers and snake-oil salesmen conveniently forget the actual science, using a few choice phrases or crafted summaries to fuel their narratives. So, before the end of Men’s Health Month, let’s see what the clinical evidence shows.
How the Male Fertility Signal Works
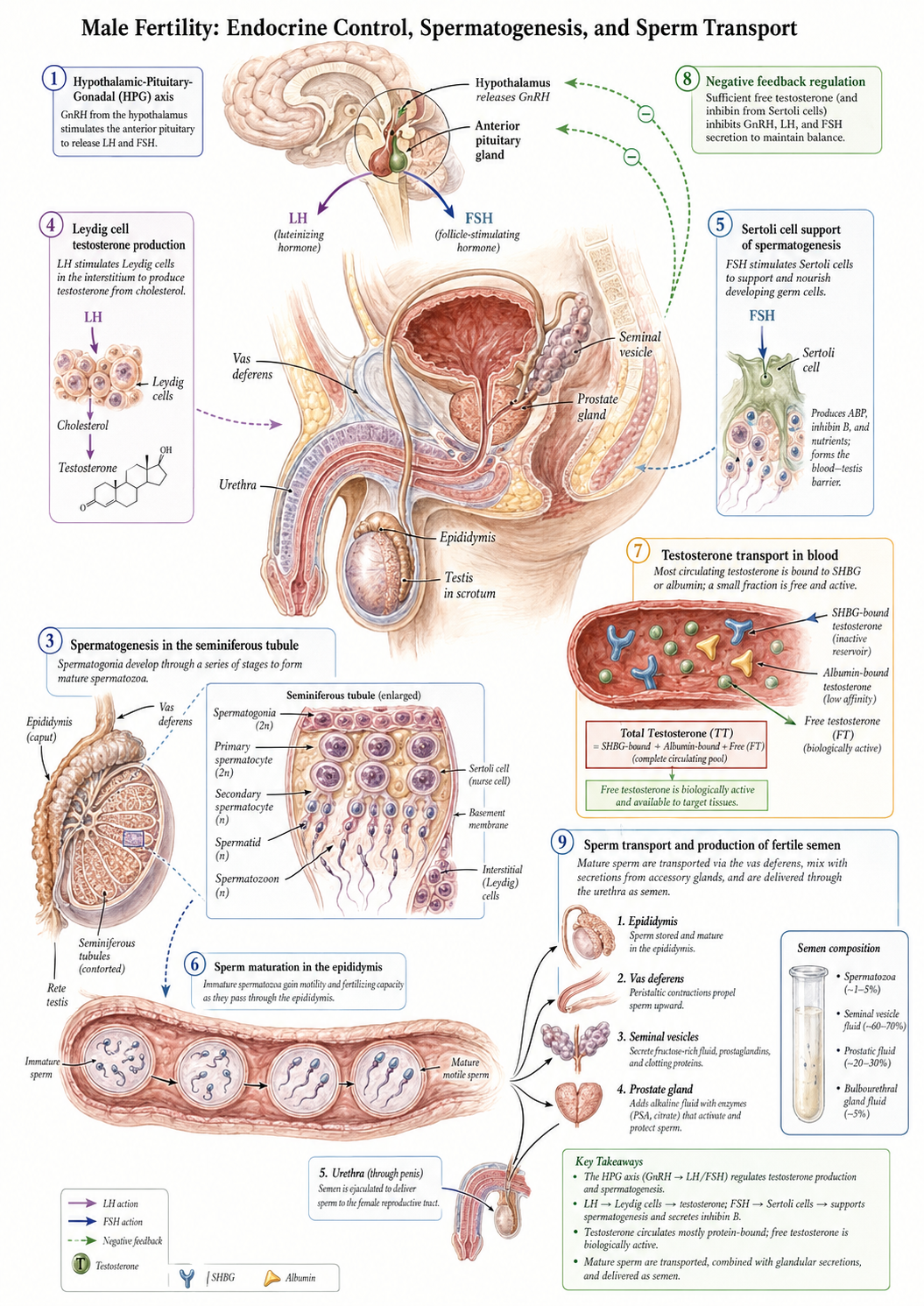
Male fertility begins with a command chain between the brain and the testes. The hypothalamus signals the pituitary gland, which releases two hormones called gonadotropins. Together, this system is called the hypothalamic-pituitary-gonadal, or HPG, axis. In men, luteinizing hormone (LH) travels through the bloodstream to the testes, where it binds to Leydig cells, prompting them to convert cholesterol into testosterone.
The total testosterone reflects the entire output of those Leydig cells; however, only a small fraction, roughly 1 to 2%, is free testosterone, unbound in the bloodstream, and the only form biologically active enough to cross cell membranes and bind to androgen receptors helping maintain muscle mass, libido, and co-driving the development of sperm.
The second signal comes from follicle-stimulating hormone (FSH), the other co-driver, which targets Sertoli cells in the testes to support and mature developing sperm cells, a process called spermatogenesis.
To complete the feedback loop, rising levels of free testosterone dial back the production of LH and FSH; too low a level increases their production.
Another key regulator is sex hormone-binding globulin, or SHBG, a protein made by the liver. SHBG binds tightly to testosterone, reducing the amount available as free testosterone. Too much SHBG can lower free testosterone; too little, which is common in metabolic syndrome and insulin resistance, can alter testosterone availability and clearance. In that sense, SHBG acts less like an on-off switch and more like a buffer, helping determine how much testosterone is actually available to tissues involved in libido and sperm production.
Hormones set the fertility signal, but sexual function also depends on whether blood vessels and nerves can carry out the physical response.
The Vascular Plumbing of Sexual Function
With our hormonal system primed, our autonomic system controls the plumbing. Parasympathetic “go” signals trigger a biochemical cascade in the vascular bed of the penis. These signals release nitric oxide, which relaxes smooth muscle in the penile arteries, allowing blood to flow into the corpora cavernosa, the paired erectile chambers of the penis. As those chambers fill, a fibrous sheath compresses the veins that would normally drain blood away. Blood enters, outflow slows, and the tissue becomes rigid.
The “stop” side of the system, involving our sympathetic nerves, is more complex, but one important player is phosphodiesterase type 5 (PDE5). By breaking down a signaling molecule that keeps smooth muscle relaxed, PDE5 helps the arteries constrict and allows venous drainage to resume. That is why common erectile dysfunction medications work by blocking PDE5: they prolong the chemical signal that supports blood flow.
Obesity and diabetes can affect fertility on multiple fronts: hormones, sperm production, nerves, and blood vessels.
Fertility and obesity
Male infertility can stem from a diverse array of structural blockages, genetic anomalies, or environmental stressors. Obesity and type 2 diabetes are especially important because they can contribute to secondary hypogonadism, a state in which the brain’s signal to the testes is suppressed. Excess adipose tissue can also increase the conversion of testosterone into estradiol, shifting the hormonal environment away from sperm production. They are true endocrine disrupters. With the rise in the use of GLP-1s researchers have begun asking whether these drugs might improve fertility-related outcomes by improving metabolic health.
In men with obesity-related functional hypogonadism, excess fat tissue can increase aromatase activity, converting more testosterone into estradiol, while inflammation and insulin resistance further suppress the HPG axis. Diabetes can add another layer of injury. Long-standing diabetes often damages nerves, most visibly as numbness in the feet or problems with balance, but it can also affect the autonomic nerves that help coordinate erections.
This is where GLP-1s enter the story, as drugs that may improve metabolic conditions that disrupt the reproductive system.
GLP-1s and Hypogonadism
A small study found that GLP-1s administered to overweight or obese men with diabetes improved testicular function, primarily through weight reduction and by rebalancing the suppression of the HPG axis caused by obesity. There were increases in total and free testosterone, LH, and FSH, all of which were rebalanced by SHBG. Researchers also noted that the use of GLP-1s in these patients improved self-reported erectile function. As an interesting aside, testosterone use is commonly associated with suppression of LH and FSH, so it seems to me that the GLP-1s may be exerting their greatest impact on SHBG to reset the HPG axis.
The Swimmers: Sperm Count, Motility, and DNA Integrity.
GLP-1 receptors have been found in the testes and appear to be involved in the energy metabolism required for spermatogenesis. Studies have shown that obese men are more likely to have low sperm counts, in part due to increased estrogen and reduced testosterone levels associated with excess fat. Insulin resistance and inflammatory markers, both linked to obesity, appear to reduce sperm motility, the ability of sperm to swim, and increase sperm DNA fragmentation, a form of genetic damage within sperm cells.
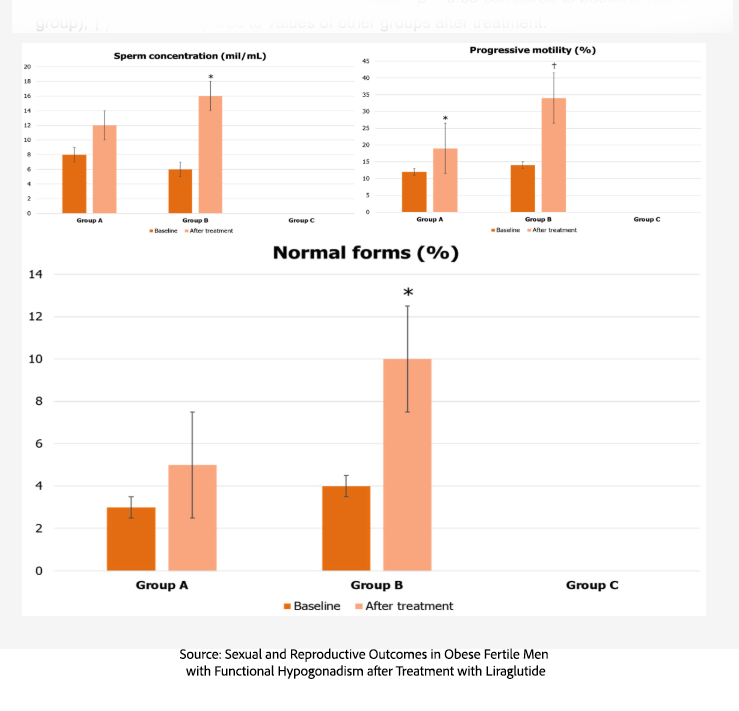 A study of 110 men of childbearing age (18–35 years) with metabolic hypogonadism compared three approaches: gonadotropin therapy (A), GLP-1 therapy (B), and testosterone therapy (C). In that study, the GLP-1 group showed greater improvement in sperm count, motility, and morphology—the percentage of sperm with normal shape—than the comparison groups.
A study of 110 men of childbearing age (18–35 years) with metabolic hypogonadism compared three approaches: gonadotropin therapy (A), GLP-1 therapy (B), and testosterone therapy (C). In that study, the GLP-1 group showed greater improvement in sperm count, motility, and morphology—the percentage of sperm with normal shape—than the comparison groups.
A small study of 26 lean, normal-weight men ages 18 to 50 with normal hormone profiles and satisfactory sexual function found no meaningful changes in hormones, sexual desire, or sperm characteristics during GLP-1 use. That is an important counterpoint: GLP-1s may have the clearest reproductive effects in men whose fertility hormones are already disrupted by obesity or metabolic disease, not in otherwise healthy men seeking enhancement.
While the sperm data are encouraging in metabolically unhealthy men, the erection data are less straightforward.
One medical-record study of more than 10,000 men with type 2 diabetes compared those starting a GLP-1 receptor agonist with those starting a DPP-4 inhibitor, another diabetes drug that affects incretin signaling (A DPP-4 inhibitor will increase GLP-1 levels). The initial analysis suggested a modest worsening in erectile-function outcomes, but that difference disappeared after more careful adjustment of the comparison group. By contrast, a cardiovascular-outcomes study of more than 5,300 men with diabetes found a modest protective association, with slightly fewer new cases of erectile dysfunction among men receiving a GLP-1 compared with placebo. For now, the fairest conclusion is that GLP-1s may improve the hormonal setting for fertility in some men, while their effects on erections remain uncertain.
Metabolic Treatment, Not Fertility Magic
When we look beyond the social media noise and examine the clinical data, the true value of GLP-1 receptor agonists in male reproductive medicine becomes clear. For men with obesity-associated functional hypogonadism, these medications offer a fertility-preserving therapeutic option. While evidence for resurrecting compromised vascular plumbing remains mixed and awaits larger trials, GLP-1s rescue the brain-testicular feedback loop from the grip of adipose tissue. As with many obesity related diseases, GLP-1s are rewriting the script for modern male reproductive health.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


