
The CDC Study
The CDC studied non-COVID mortality [1] in a cohort of 11 million persons from seven electronically linked sites.[2] They considered members who received one or both shots of Pfizer or Modena vaccines or the J&J vaccine. Data on cause of death, vaccination status, age, race, ethnicity, timing, and site were obtained on 6.4 million individuals matched with 4.6 million controls. The outcome was the time, in person-years, between vaccination and their death. About nineteen thousand deaths occurred from December 14, 2020, to July 31, 2021.
- They found no evidence that vaccination might increase risks for other causes of death.
- All vaccinated racial and ethnic groups had significantly lower non-COVID mortality risks than the unvaccinated comparison group. Non-Hispanic Asians had the lowest mortality overall.
- There was no difference by gender.
CDC concluded that the study
“reinforces the safety profile of currently approved COVID-19 vaccines in the United States.”
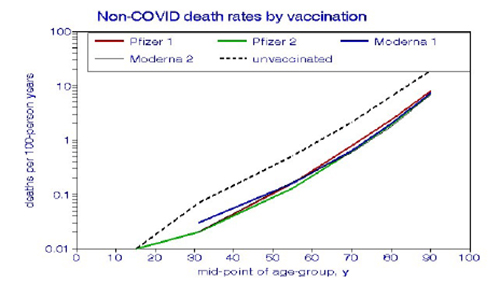 An Alternative Analysis. The CDC analysis compared mortality risks by age or demographic subgroups but, for simplicity, we considered age as a continuous risk factor. The J&J vaccinated had too few subjects for this modeling approach. As apparent from the graph, the mortality differences between Pfizer and Moderna were insignificant, only 0.4%. By contrast, COVID vaccination reduced adult non-COVID mortality by about a factor of 3. Given the short time course of the study, roughly seven months, these relationships are essentially acute.
An Alternative Analysis. The CDC analysis compared mortality risks by age or demographic subgroups but, for simplicity, we considered age as a continuous risk factor. The J&J vaccinated had too few subjects for this modeling approach. As apparent from the graph, the mortality differences between Pfizer and Moderna were insignificant, only 0.4%. By contrast, COVID vaccination reduced adult non-COVID mortality by about a factor of 3. Given the short time course of the study, roughly seven months, these relationships are essentially acute.
Why did vaccination confer protection against deaths unrelated to COVID?
Could the decision to vaccinate have been more critical than the vaccination itself?
How Effective are the Vaccines?
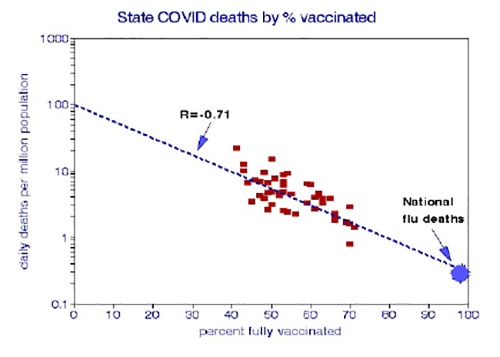 The CDC analysis contrasted the risk of vaccinated and unvaccinated groups, not the efficacy of vaccination in preventing infection. I estimated that relationship by comparing average COVID-19 state-level daily mortality rates among states, for which vaccination rates ranged from 40 to 80%. [3]. This relationship is highly statistically significant, with a (negative) correlation coefficient of 71%.
The CDC analysis contrasted the risk of vaccinated and unvaccinated groups, not the efficacy of vaccination in preventing infection. I estimated that relationship by comparing average COVID-19 state-level daily mortality rates among states, for which vaccination rates ranged from 40 to 80%. [3]. This relationship is highly statistically significant, with a (negative) correlation coefficient of 71%.
- Total vaccination of the population might be required to reduce COVID-19 mortality rates to the endemic levels experienced for influenza mortality.
- The graph indicates a COVID mortality ratio (MR) of about 300 between those vaccinated and those not - considerably greater than the CDC estimate for non-COVID mortality (an MR of 3) or the CDC estimated ratio of COVID-related deaths (MR of 12).
I also examined relationships among states for ethnicity, household crowding, income, face-mask usage, and political preference, which I consider a proxy for mistrusting science [4]. Significant correlations among these factors include:

These correlations show that COVID-19 death rates are most closely associated with vaccination rates and that  vaccination rates are strongly associated with politics (i.e., distrust of science), as is face-mask usage. The relationship between voting Republican and not getting vaccinated is the strongest, indicating that vaccination rates could be increased by decreasing political influences. Flu vaccination had weaker protection from all-cause mortality, at about 34% [5]. However, both vaccinations were significantly correlated with the percentage of Republican voters and presumably distrusted science.
vaccination rates are strongly associated with politics (i.e., distrust of science), as is face-mask usage. The relationship between voting Republican and not getting vaccinated is the strongest, indicating that vaccination rates could be increased by decreasing political influences. Flu vaccination had weaker protection from all-cause mortality, at about 34% [5]. However, both vaccinations were significantly correlated with the percentage of Republican voters and presumably distrusted science.
Discussion and Recapitulation.
Longevity may be affected by personal characteristics (age, race, socioeconomics, smoking, exercise, etc.) and disease-specific countermeasures (medication, vaccines, and reduced exposure to infectious agents). COVID-19 infections and subsequent mortality rates are primarily affected by relative exposure to the virus and vaccines that enhance protective immune responses. Differences between vaccinated and unvaccinated patients provide clues to the relative importance of vaccinations and personal characteristics.
- State-to-state variations in COVID-19 mortality rates can illustrate personal relationships and individual decisions to vaccinate.
- State-level averages of COVID-19 mortality rates, vaccination rates, and face-mask usage are significantly intercorrelated, making it difficult to distinguish their separate effects.
- Increased vaccination rate is the best predictor of reduced COVID-19 mortality.
- Distrust of science, as captured by political affiliation, is the best predictor of reluctance to vaccinate against COVID-19.
- Influenza vaccination rates are lower in Republican states, indicating that this distrust may not be limited to COVID-19.
Increasing full vaccination coverage from the present 58% to a herd-immunity goal of 75% would require reducing the proportion of science doubters from the current 50% to about 20%, an improbable scenario. We learned that downgrading COVID-19 to endemic status is problematic at this time.
[1] MMWR Early Release Report 70, October 21, 2021.
[2] Pasadena CA, Oakland, CA, Denver CO, Portland OR, Seattle WA, Minneapolis MN, Marshfield WI.
[3] This included the contiguous United States; the District of Columbia was an outlier and not included.
[5] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8423473/pdf/ciaa1862.pdf


