There is no doubt that GLP-1s induce weight loss, with a rising percentage with each new generation targeting multiple sites in the metabolic pathways underlying obesity. But in allowing “no good deed to go unpunished,” there have been rising concerns that in the process of losing unwanted fat, we are shedding our more desirable “lean.” Could muscle wasting and loss of strength endanger our lives in some unintended manner?
As it turns out, a new study in Cell Reports Medicine suggests these concerns may have been a byproduct of imprecise measurement rather than biological reality. This investigation combined four studies on diet-induced obese mice with a 12-week proof-of-concept clinical trial involving ten middle-aged human participants with obesity and diabetes.
What is "Lean," Anyway?
To understand the “math of loss,” we begin with a common body-composition tool: dual X-ray absorptiometry, or DXA. DXA uses high- and low-energy X-ray beams to distinguish bone, fat, and lean tissue based on their absorption patterns. It is good at separating fat from non-fat mass. But that non-fat category is broad. It includes organs, connective tissue, body water, and muscle. As a result, lean body mass, or LBM, is not simply a measure of muscle.
That distinction matters because some of the “lean” tissue lost during weight loss may come from organs carrying excess fat, especially the liver.
Moreover, a majority of obese individuals develop an inflammatory response to fats increasingly stored in their liver, leading to metabolic-dysfunction-associated steatotic liver disease (MASLD). 20-30% progress to a more severe form known as MASH (Metabolic-dysfunction-associated Steatohepatitis), in which the liver is actively damaged.
Weight-loss diets reduce both fat and lean body mass (LBM), though to varying degrees. The “rule of thumb” in traditional dietary weight loss is that LBM accounts for only about 25% of overall weight loss. Early studies of GLP-1s suggested higher percentages, around 40%, which raised concern. But if LBM includes more than muscle, a high percentage of “lean” loss does not automatically mean a high percentage of muscle loss.
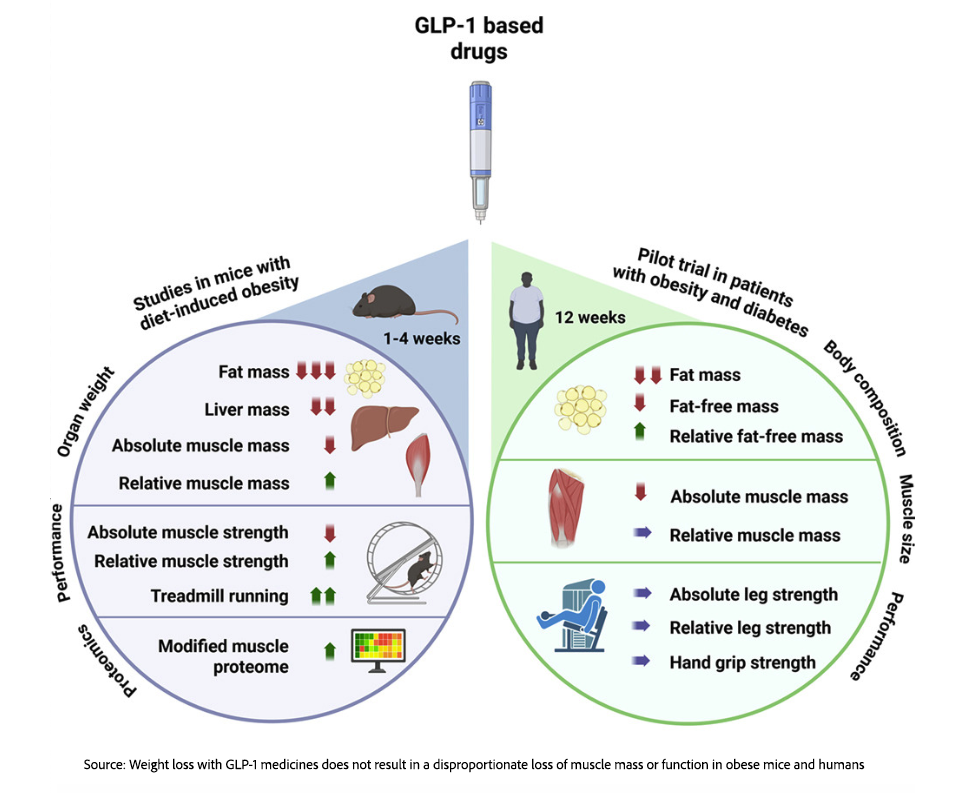
In the current study, the mice had nearly twice as much LBM as fat mass before the various GLP-1 interventions. Although the extent of fat and LBM loss varied by drug, dosage, and treatment duration, LBM loss accounted for 20-32% of total weight loss. In the proof-of-concept human trials, LBM loss was roughly 30% of the total. More importantly, much of that weight loss occurred in the liver, as it sheds unhealthy internal fat, suggesting a new treatment path for both MASLD and MASH.
Muscle mass declined, but by much less than lean-body-mass numbers alone might suggest. Even in the most extreme case, when one leg was immobilized in a cast and muscle loss was driven by disuse, muscle mass fell by about 13% to 24%. That was comparable to the loss seen with simple calorie restriction, suggesting that GLP-1 treatment itself was not uniquely wasting muscle.
The bottom line is that GLP-1s promote more fat loss than muscle loss and that the concern about “too much” muscle wasting is unnecessary.
Ratios: Why the Muscle-to-Body-Weight Ratio Matters
Because fat loss exceeds muscle loss, the ratio of muscle mass to total body weight can shift in a favorable direction. Even if muscles become slightly smaller, they have less body weight to move. In practical terms, the power-to-body-weight ratio may improve, which helps explain why mobility and physical function can improve even when absolute muscle mass declines.
Obese mice in the treatment groups were able to keep pace with the slimmer controls, showing increased time to exhaustion and total distance covered. In the abbreviated human trial, despite a decrease in the cross-sectional area of their thigh muscles, they maintained their absolute and relative leg strength. That finding is preliminary, but it supports the idea that function may matter more than muscle size alone.
Exercise Sends a Signal Muscles Need
Further investigation sought to understand how pharmacological weight loss might differ from simple calorie restriction. In one experiment, mice had one limb immobilized with a cast and were either given a GLP-1 medication or subjected to caloric restriction. GLP-1 medications induce distinct molecular changes in muscle that differ from those seen with simple calorie restriction, even when weight loss and calorie intake are identical.
In active limbs, these drugs increase mitochondrial protein levels to enhance energy production, whereas in immobilized limbs, the molecular focus shifts toward remodeling and quality-control pathways. Because muscle loss during inactivity is comparable to that seen with standard dieting, GLP-1s do not specifically target muscle tissue; instead, atrophy is driven by total weight reduction and a lack of physical demand.
This underscores the essential role of exercise, which provides the biological signal needed to preserve muscle mass, as evidenced by studies showing that active limbs often maintain or even increase relative to body weight.
Less Panic, More Precision
GLP-1s reduce both fat and lean mass. However, the mild loss of lean mass is a healthy trade-off for the more significant reduction in fat mass. Moreover, the reduction in lean mass seems to help reduce inflammation associated with MASLD and MASH – an additional, unanticipated benefit. That said, GLP-1s are not magic bullets. If people lose weight while remaining inactive, their muscles have little reason to stay strong. Even modest exercise can help preserve function by signaling to muscles that they are still needed.
A more nuanced takeaway is that biological ratios can matter as much as absolute numbers. A measurement such as “grams of muscle” tells us something, but not everything. In a complex adaptive system like the human body, function depends on relationships among parts: muscle, fat, liver health, strength, mobility, and physical demand. A smaller body with slightly smaller muscles may still move better, perform better, and face lower metabolic risk. That does not mean muscle loss should be ignored. It means the GLP-1 muscle loss needs a more precise question: not simply “How much lean mass was lost?” but “What was lost, from where, and did function suffer?”
Source: Weight loss with GLP-1 medicines does not result in a disproportionate loss of muscle mass or function in obese mice and humans Cell Reports Medicine DOI: 10.1016/j.xcrm.2026.102665

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


